
It’s funny how the same old hysterical drug myths refuse to die. Back in 1992 former editor of the Journal Addiction Research & Theory John Booth Davies described the persistent tale of pushers and helpless addicts:
“At the present moment, the standard line taken by a majority of people in the media, in treatment agencies, in government and elsewhere, hinges around notions of the helpless addict who has no power over his/ her behaviour; and the evil pusher lurking on street comers, trying to ensnare the nation’s youth. They are joined together in a deadly game by a variety of pharmacologically active substances whose addictive powers are so great that to try them is to become addicted almost at once. Thereafter, life becomes a nightmare of withdrawal symptoms, involuntary theft, and a compulsive need for drugs which cannot be controlled. In fact, not one of these things is, or rather needs to be, true.”
– from The Myth of Addiction by John Booth Davies, 1992
When the anti-drug crowd of the 1980s peddled such tales, we recognized it as hysterical nonsense. But why then do we accept it from Stephen Colbert? In a recent 4 and a half minute segment titled “Colbert Links Big Pharma’s Sackler Family To America’s Opioid Crisis” he repeats all the myths Davies highlighted above, and more. Basically, Colbert has simply taken the typical drug scare narrative from the 1980s, and swapped out crack for oxycontin, then replaced ghetto drug dealers with doctors and pharmaceutical companies. History has shown the crack scare was misguided, and the opioid scare will look even more foolish in hindsight.
I’ve been disappointed to see many friends sharing it and expressing their agreement. Have a look, and see if you can spot all the drug myths. I’ll explain them below:
Now I don’t blame him, because he didn’t create this narrative, he’s just parroting it. But the video has gone viral, which means that people are eating it up. On Colbert’s Facebook page, where most of his videos get around 150,000 views, his opioid crisis video is already up to 3 million views in less than a week. It’s upsetting to see people lap up this garbage.
Understanding the drug myths mindlessly repeated by Stephen Colbert
Myth #1: Opioids have a quality of “addictiveness.”
Colbert complains that the Sackler family and their company Purdue, makers of Oxycontin, “downplayed the risk of addiction associated with opioids,” and then he says outright that the opioid crisis “is their fault. This implies that the Sacklers are “drug pushers” and that the drugs they’re “pushing” are inherently addictive. But the entire idea of “addictive drugs” is nonsense – it amounts to the idea that a drug has the power to enslave someone, to force them to continue to use the drug against their will. Thus, exposure to the drug is like exposure to a pathogen – you catch addiction like one catches a cold. There’s a big problem here though: why do so many people who are exposed to the pathogen of prescription opioids fail to become addicted?
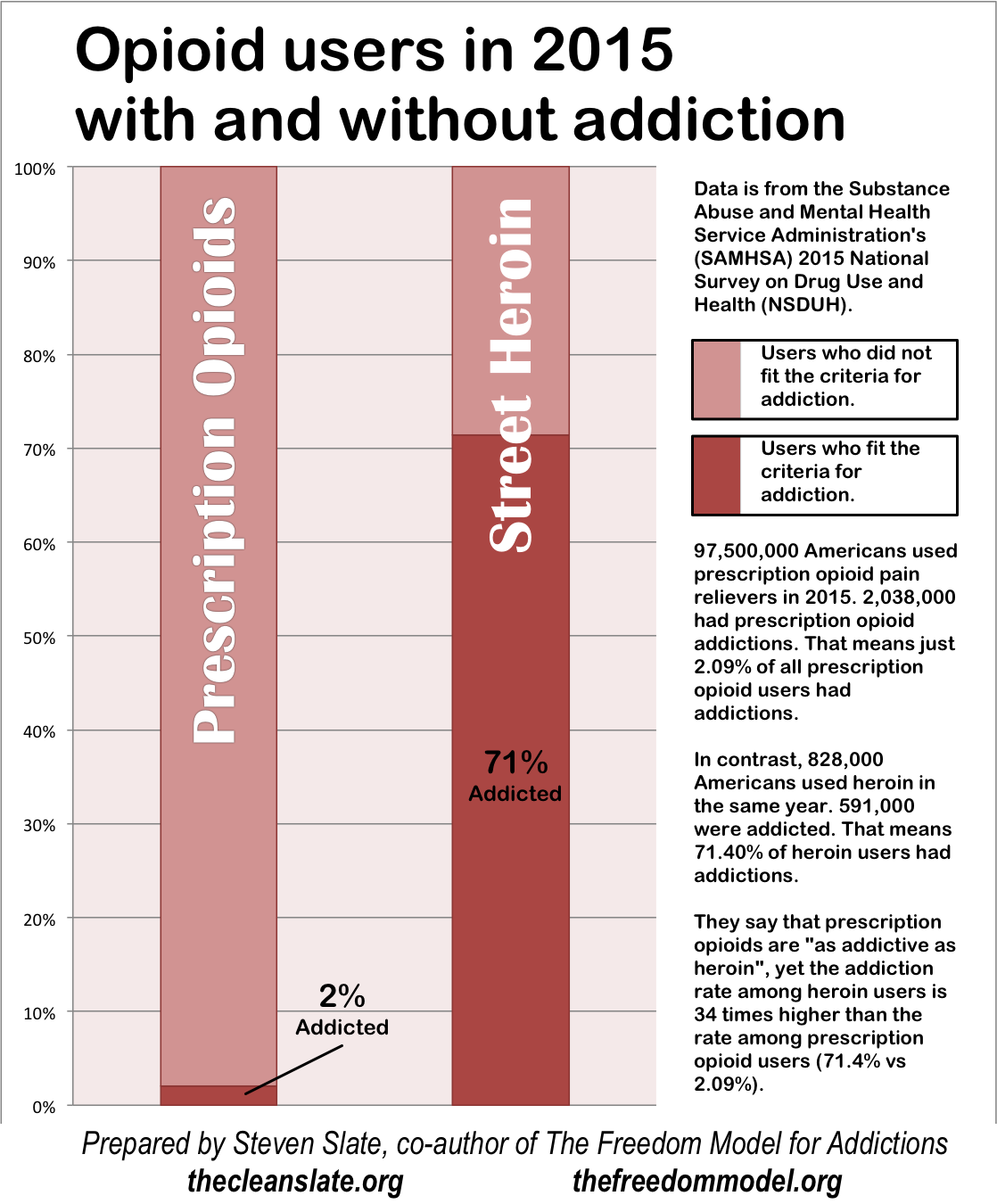
In 2015, 97.5 million Americans used prescription opioids – but only 2 million fit the criteria for addiction (SAMHSA). Why are only ~2% of the people exposed to this pathogen in a year sick with its disease? Well, logic would dictate that it ain’t really a pathogen. Maybe something else is at the root of why some people use these drugs in extreme ways.
Columbia University neuroscientist Carl Hart writes that “The vast majority of opioid users do not become addicts. Users’ chances of becoming addicted increase if they are white, male, young and unemployed…” What type of pathogen chooses its victims by employment status? Why is a drug “addictive” to the unemployed, while being “non-addictive” or “less addictive” to those with stable careers? Because the drug doesn’t contain a quality of addictiveness. A person attaches themselves to a drug, by virtue of being enamored with it’s effects, by looking to it as a solution – the beauty (addictiveness) is in the eye of the beholder.

I know most readers are still skeptical though. Consider this as well – they say the prescription opioids are equivalent to heroin, and they are correct. But if this is the case, why does heroin seem to “addict” a much higher percentage of its users? In 2015, there were 828,000 Americans who used heroin, while 591,000 of them fit the criteria for addiction (SAMHSA, NSDUH 2015).
The prescription opioids and heroin are nearly identical – they all bind to and stimulate the opioid receptors. Why then are a paltry 2% of prescription opioid users addicted while a whopping 71% of heroin users are addicted? Because again, it’s not about the pharmacology of the drugs – addiction is about the motivations of the user. People who use heroin are willing to break the biggest drug taboo in order to get what is supposed to be the best high. The high rate of addiction to heroin is a function of its users, and the low rate of addiction to prescription opioids is a function of its users. That is to say, most people use prescription pain relievers looking for nothing more than relief of physical pain. Pharmacology has nothing to do with the gap in addiction rates between these drugs..
Here’s a chart I put together with this data. It helps to visualize it:
Don’t take that as evidence that heroin is “more addictive” than prescription opioids. It isn’t. The point is that neither are addictive. They’re the same thing, and we even have a real world test with medical use of heroin, as addiction researcher Bruce K Alexander wrote:
“In the U.K., heroin was widely used as a medication for cough, diarrhea, chronic pain from the beginning of the 20th century to the present. In the year 1972, for example, British physicians prescribed 29 kilograms of heroin—millions of doses—to medical patients. A major portion of this heroin is sold as an ingredient in cough syrups which are readily available. Careful examination of the British statistics on iatrogenic addiction ten years later revealed “there is a virtual absence of addicts created by this singular medical practice” (Trebach, 1982: p. 83).”
Myth #2: Drugs are bad.
What happened to the other 95.5 million americans who used prescription opioids in 2015? Oh I don’t know, maybe THEIR PAIN WAS EFFECTIVELY TREATED.
For thousands of years, opiates were the only effective painkiller known to man. In fact, they were the only effective class of any medication. They helped with physical pain, they suppressed deadly coughs, they prevented death by bowel problems and dysentery, and they generally eased the painful deaths of people all over the world. To this day they remain the most effective pain medication available.
Yet Colbert has the gall to mock the opioids in his segment by rewriting the hippocratic oath to read “First do no harm. Unless harming is extremely profitable! Then harm! harm! harm!”
It’s funny, as long as you are either callous or ignorant. It’s dangerous, because it’s helping to get the nation swept up into a hysteria against the world’s oldest and most effective class of medications.
Colbert’s tone suggests that we all just know opiates are bad. That’s easy to believe given the current talk of overdoses. But even the overdose spike is not quite what it seems. As Columbia University neuroscientist and drug researcher Carl Hart writes in an article for Scientific American titled People Are Dying Because of Ignorance, not Because of Opioids, the overdose risk of opioids is overhyped and misrepresented:
“It is certainly possible to die from an overdose of an opioid alone, but this accounts for a minority of the thousands of opioid-related deaths. Many are caused when people combine an opioid with another sedative (such as alcohol), an antihistamine (such as promethazine) or a benzodiazepine (such as Xanax or Klonopin). People are not dying because of opioids; they are dying because of ignorance.”
Ken Anderson of the HAMS harm reduction organization has reviewed the available data on drug overdose/poisoning deaths in the US and concludes that over 90% involve the kind of drug mixing mentioned by Hart.
It’s not that opioids are especially bad, it’s that right now many people are using them in an especially bad/dangerous way, including by mixing them with other drugs.
Myth #3: Prescription opioid pain relievers are a gateway drug to heroin.
As Colbert says, “four out of five new heroin users started by misusing prescription painkillers…”, this might be true in the current moment, and I’ll agree with it for argument’s sake. But so what? The National Safety Council whom Colbert cited for the 4 out of 5 stat also says that “Studies show 4% to 6% of opioid misusers will transition to heroin.” Misusers are already a fraction of users, and then we take 4 to 6% of that number? It must be an extremely exclusive gateway, since barely anyone gets through it.
Even NIDA admits this gateway theory ain’t all it’s cracked up to be, in their report on the connection between these drugs they say that:
“While prescription opioid abuse is a growing risk factor for starting heroin use, only a small fraction of people who abuse pain relievers switch to heroin use. According to general population data from the National Survey on Drug Use and Health, less than 4 percent of people who had abused prescription opioids started using heroin within 5 years (Muhuri et al., 2013). This suggests that prescription opioid abuse is just one factor in the pathway to heroin.” (NIDA: Prescription Opioids and Heroin PDF archived)
And then they show that the correlation has gone in both directions over time, with the chart below that indicates the percentages of addicts who started with prescription opioids or heroin over the decades:
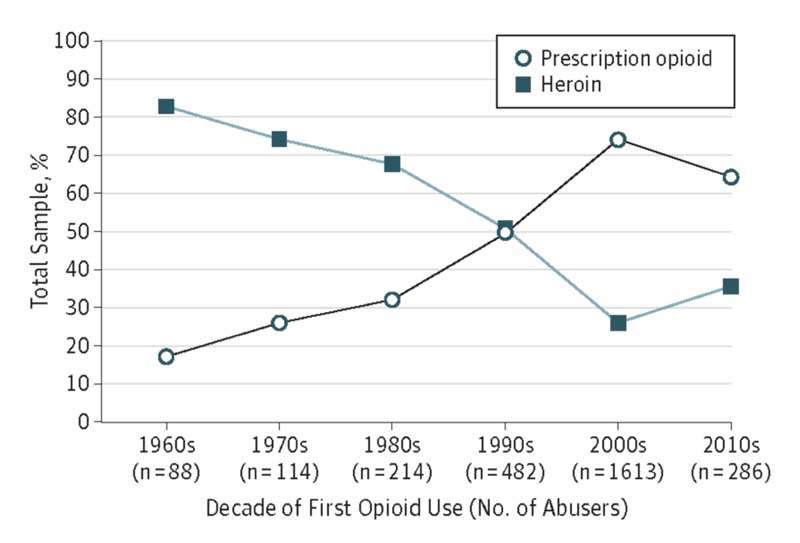
I was a heroin “addict” myself (see my TEDx Talk on it), and the first opioid I had was heroin. I suppose prior to the 90’s you could’ve called heroin a gateway to prescription opioids based on the data above. It appears people pass both directions through this gateway depending on the fashions of the time. But Colbert’s citation of the 4 out of 5 stat makes it appear like heroin use is purely a function of prescription opioid marketing. And the point is what? To suggest that we should do away with prescription opioids? This is absurd and dangerous. There were less than 600,000 heroin “addicts” in the same year that 95.5 million americans used prescription pain relievers uneventfully, and to their benefit.
Myth #4: Opioid pain relievers are “pushed” on unwilling users.
The Sacklers and their company Purdue are all portrayed as drug pushers. The world has had opioids for thousands of years. The world has had oxycodone (the key ingredient of oxycontin), since 1917! But according to Colbert, the Sacklers are going to get the world hooked on opioids all of a sudden, and they are to be equated with Pablo Escobar??? Again, this bit is funny from some perspective, but reckless in the ignorance & misinformation it’s spreading. Moreover, doctors are a key part of the pipeline, as they do the prescribing. So what do we know about people becoming “accidentally addicted” and turned out by their unscrupulous doctors who serve as the street dealers for the Sacklers?
As Maia Szalavitz puts it, writing for Columbia Journalism Review the naive person accidentally addicted by an overprescribing doctor is a tale the media wants to tell, and wants to be true, but it just doesn’t fit the facts:
…reporters downplay their subjects’ earlier drug misuse to emphasize the role of the medical system, as seen in this piece from the Kansas City Star. The story, headlined “Prescription pills; addiction ‘hell,’” features a woman whose addiction supposedly started after surgery, but only later mentions that she’d previously used crystal meth for six months.
Yet here are the facts (also from Szalavitz):
While some people become addicted after getting an opioid prescription for reasons such as a sports injury or wisdom teeth removal, 80 percent start by using drugs not prescribed to them, typically obtained from a friend or family member, according to surveys conducted for the government’s National Household Survey on Drug Use and Health. Most of those who misuse opioids have also already gone far beyond experimentation with marijuana and alcohol when they begin: 70 percent have previously taken drugs such as cocaine or methamphetamine. [emphasis added]
And as CATO Senior Fellow Jeffrey Singer writes:
“…2010 and 2012 Cochrane systematic analyses show chronic non-cancer pain patients on opioids have a roughly 1 percent addiction rate, and a January 2018 study by researchers at Harvard and Johns Hopkins of more than 568,000 “opioid naïve” patients over 8 years who were given opioids for acute postoperative pain showed a total “misuse” rate of 0.6 percent. In a 2016 New England Journal of Medicine article, Dr. Nora Volkow, the Director of the National Institute on Drug Abuse, stated, “Addiction occurs in only a small percentage of patients exposed to opioids—even those with preexisting vulnerabilities.”
What all of this also indicates is that you can’t push drugs on people. The entire notion of pushing rests on the myth of addictiveness – that once you can trick a person into trying the drug, they won’t be able to stop. Drugs possess no such quality. The person who continues to use is always a willing participant.
Furthermore, let’s just think like greedy damn capitalists for a minute. If you can sell your drug to 95.5 million non-problem-users a year, how does it make sense to nefariously “push” the drug on 2 million users who? Why jeopardize the money you’re making by pushing? Would the heat brought by the overdoses deaths and other problems really be worth the extra 2 million customers? It’s just absurd on it’s face. I know Colbert cites the fact that they pleaded guilty to something – but I also know that plenty of people plead guilty to crimes they didn’t commit in order to strike a plea deal. I’ve done it myself back in my “addict” days. Plenty of companies settle cases in which they do not believe they’re in the wrong, just so that they can move on and avoid the spectacle of a trial. Purdue apparently “downplayed” the abuse potential of oxycontin. But I’d say abuse potential is a damn debatable concept in and of itself.
The bottom line is that the vast majority of stuff being flung at the drug companies in the case of opioids is mud. It’s being flung by people so ignorant, that as a bonus, they’d throw in this last myth…
Myth #5: Meth mouth.
In another joke that’s funny only if you’re ignorant and full of misinformation, Colbert says that the Sacklers’s selling of both brand-name and generic oxycontin is equivalent to selling both methamphetamine and “Tooth-Looseners.”
This has long been debunked – see The Meth Mouth Myth, Our Latests Moral Panic in Slate magazine from 2009. Meth has no special tooth decaying quality that isn’t possessed by plenty of other everyday drugs such as blood pressure pills or vitamin c tablets among others. And, the decay is extremely rare. As drug researcher Carl Hart writes:
There is no empirical evidence to support the claim that methamphetamine causes physical deformities. Of course, there have been the pictures of unattractive methamphetamine users in media accounts about how the drug is ravaging some rural town. The infamous “meth mouth” images (extreme tooth decay) have been widely disseminated. But, consider this: methamphetamine and Adderall are essentially the same drug. Both drugs restrict salivary flow leading to xerostomia (dry mouth), one proposed cause of “meth mouth.” Adderall and generic versions are used daily and frequently prescribed – each year they are among the top 100 most
prescribed drugs in the United States – yet there are no published reports of unattractiveness or dental problems associated with their use. The physical changes that occurred in the dramatic depictions of individuals before and after their methamphetamine use are more likely related to poor sleep habits, poor dental hygiene, poor nutrition and dietary practices, and media
sensationalism.
There you have it. Colbert spread 5 big drug myths in 4 and a half minutes, and it’s been seen by millions of people. The truth needs to be seen by millions of people too.
The truth can set people free from drugs.
As psychologist and addiction researcher Stanton Peele has long said, the belief in addiction is what makes people feel addicted. I know this can be a hard pill to swallow but it’s true. Yes, opioids use can lead to physical withdrawal symptoms upon stopping, but this doesn’t force anyone to keep using. In fact, most people who’ve gone through opioid withdrawal didn’t even know. The typical surgical patient on morphine through the last century just thought they were sick when they were discharged from the hospital and withdrew from the morphine at home. That withdrawal traps people is yet another myth long debunked. It’s also a good example of how addiction is a learned experience, and can be unlearned. I discuss all this in the book I co-authored, The Freedom Model for Addictions: Escape the Treatment and Recovery Trap. It shows people how to let go of the addict identity and reclaim their power of choice over substance use. I get plenty of feedback from people who used the book to get over their substance use problems without any meetings or treatment.
You can also learn the Freedom Model approach in private online classes, or at the Freedom Model Retreat.
Thank you very much for debunking these propaganda talking points. It’s insane how people are just swallowing this wholesale. Did you know there’s a new bill moving forward in the U.S. House – HR 6 – that will limit the percentage of opioid pain medication hospitals can use for any reason? Imagine being a post-operative patient denied pain relief (it’s happening) because the hospital has to guess how many other patients might need it instead. I guess the general public prefers to follow the misinformed parrots like Colbert – until they finally figure out this anti-Rx-opioid hysteria will impact them too.
What everyone forgets is that before this so-called “opioid crisis” there was a very real crisis involving the gross undertreatment of pain – there was a WHO report and a Congressional Declaration about it. I know a nurse who remembers cancer patients dying in agony back then and she’s very concerned those days are returning. The ball is rolling in that direction. I live with severe pain and need effective pain management. For me that’s come to include reasonable doses of opioid-based medication. I’m sick of being subject to random drug tests (which I and my insurance must pay for) and the invasion of privacy that comes with prescription drug monitoring programs. I truly live in fear that my PM doctor (who is burning out) will retire bc very few of them remain. Other pain patients haven’t been so lucky. If their doctors quit prescribing pain meds or quit the field of pain management (this is happening a lot), then patients are abruptly yanked off these medications, or if an insurer imposes quantity limits below the level that’s been working, these people can go into physical withdrawal. They tough it out on their own or they get sent to rehab (which brands them since few doctors will risk prescribing pain medication with that track record). And then they’re left to deal with that pre-existing painful condition using SCAM treatments “supplemental complementary alternative medicine” (many untested or with highly variable efficacy related to the cause). Or, if they’re lucky, with suboxone which isn’t all that effective for pain.
I know your blog is aimed at dealing with substance use concerns, but this is an important fallout of the “opioid crisis”. You might also be interested to note the extent of addiction-service industry physicians involvement in opioid policy decisions (think healthcare). I suspect it’s because pain patient clients will improve rehab “results” since their experiences are most likely limited to physical withdrawal aspects (and since they were never addicted, they also aren’t likely to show “recidivism” which would bring the center’s rates down). Given the blatant conflict of interest, I don’t understand why this is allowed or why there aren’t any legal requirements for disclosing these connections. Thanks again for tackling the propaganda – it’s certainly an uphill battle.