The Misguided Obsession with Heroin / Opiate Maintenance Drugs (Suboxone, Subutex, Buprenorphine, Methadone)
Two fairly recent stories discussing Suboxone / Buprenorphine have me shaking my head. In one, a pregnant woman who had already quit using opiates was punished for refusing to take Suboxone. In another, it is claimed that Glee actor Cory Monteith wouldn’t have died from overdose, if only he had been prescribed some sort of maintenance drug for heroin addiction. I’ll discuss these, but I need to lay down a few foundational points for my thinking on this.
First, we need to know that a large majority of those who’ve used heroin and other opiates are actually recreational users. I know it’s shocking, and it’s supposed to be impossible, but this was well established in several studies analyzed by Norman Zinberg in his book Drug, Set and Setting published in 1984 by Yale University Press.
Second, we need to know that most of those whose use of heroin reaches the level classified as “addiction” or “dependence” eventually get over their addiction. In the two studies by Lee Robins, only 15% and 12% remained addicted long term (cited by Gene Heyman in Addiction: A Disorder of Choice, 2009, Harvard). Other large studies showed that 60-75% of heroin addicts can be found to have gotten over their addiction.
Thirdly, we need to know that those who get treatment for drug addictions usually fare worse than those who don’t receive treatment.
Heyman did an important thing. He showed that most research that looked only at addicts who get treatment showed dismal success rates, and relapse rates from 50-90%. Then he showed the wider research that looked at the entire population of addicts – both treated and untreated – where it’s clear that the vast majority of addicts (mostly untreated) get over their addictions. In the case of heroin addiction it was well over 80% in the two Robins studies, and for all opioids, it was 75% in the NESARC Study, and 60% in the ECA Study. In each of those studies, only a small minority of substance dependent people were treated – most recovered without treatment.
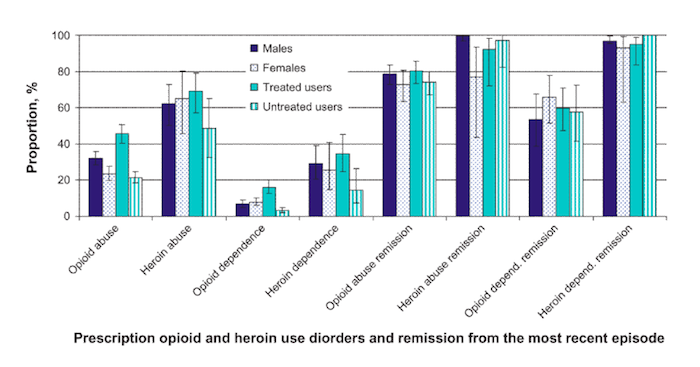
More recent results from the NESARC data show that well over 90% of those categorized as heroin abusers or heroin dependent are currently “in remission.” LINK In these results, those who had ever been treated had slightly lower rates of remission. Although I can’t find the exact number in the study, one of the graphs appears to show that 100% of untreated heroin addicts (those classified as heroin dependent), are currently in remission! Check the graph yourself – in the category all the way to the right:
Wu, L.-T., Woody, G. E., Yang, C., Mannelli, P., & Blazer, D. G. (2011). Differences in onset and abuse/dependence episodes between prescription opioids and heroin: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Substance abuse and rehabilitation, 2011(2), 77–88. doi:10.2147/SAR.S18969
The study also found that:
among individuals with PO [prescription opiate] abuse, those with a history of substance abuse treatment, on average, reported a lengthier abuse episode (41 months vs 23 months) and duration between first use and remission from the most recent episode (8.3 years vs 5.3 years) than the untreated; this difference was even more distinct among individuals with heroin abuse (treated, 83 months; untreated, 17 months) or dependence (treated, 69 months; untreated, 17 months).
So it appears that those who get treatment end up having addiction “episodes” that last longer than those who don’t receive treatment. This may be because treatment confounds the problem, and the powerlessness teachings deter attempts to change after “relapse.” Or it may not. I certainly don’t know for sure, because it doesn’t report when they actually received treatment in relation to when they achieved remission. But I do know that the higher rates of relapse for treated vs untreated individuals cited by Heyman (and many other studies) point me toward the conclusion that these longer periods of dependence and abuse may likely be caused by the ideas taught in treatment.
[For the record, Heyman himself thinks comorbid psychiatric disorders cause the treated groups to fare worse than the untreated groups- however, it was recently found in the NESARC data that “Having once experienced mood and anxiety disorders was unrelated to remission from dependence” for cocaine, nicotine, alcohol, and cannabis. That is, there was no correlation between having these major classes of comorbid disorders and success or failure in resolving a substance use problem. Related information was not provided for heroin use, but there’s no reason to assume it’s different either.]
The point is, heroin addicts’ long term prognosis might be better if they stay away from treatment programs (with perhaps the exception of medical detoxification for those who truly want to initiate abstinence – but not the unwilling). At the very least, there certainly seems to be no evidence in the above that treatment is better than no-treatment.
Do Maintenance Drugs Work? (Methadone, Suboxone, Subutex)
Regardless of the results listed above, there’s no shortage of enthusiasm for heroin/opiate addiction treatments like Suboxone (a pharmaceutical treatment for opiate addiction) in our culture today. Its supporters think it’s a medical miracle. Meanwhile, most of the information I’ve found says Buprenorphine is no more successful than methadone. What’s more, the verdict on methadone isn’t so hot itself. The research is extremely limited, as another Cochrane Review noted: “there are no trials comparing methadone maintenance treatment with drug-free methods other than methadone placebo trials, or comparing methadone maintenance with methadone for detoxification only.”
Whether Buprenorphine (the main ingredient in Suboxone) works in the long term is literally unknown, as Todd Meyers reported in The Clinic and Elsewhere:
In nearly every study since 1992, the long-term outcomes of individuals treated with buprenorphine as a replacement therapy have been described as unknown, representing a major research limitation.
And chances are, as indicated by both his own study of 12 subjects (in which only one achieved abstinence for a period of months before being murdered while dealing drugs) and one of his conversations with the researchers testing the results of Buprenorphine, that it doesn’t work long term. Here are some gems of quotes from a conversation he reported verbatim:
Physician: It’s really hard to know what’s working and not working. These data say the therapy works, but with a pretty big caveat: time.
Research Assistant: But does it matter? I mean, while the kids were here they did great. When they leave, I mean, what are you going to do?
Physician: The drug works— but in the long term things begin to fall apart.
Was Cory Monteith’s death caused by a lack of medication?
Some commentators are literally obsessed with maintenance medications. In discussing the overdose death of Glee actor Cory Monteith, Maia Szalavitz rightly points out that he was a victim of “tough love”, and that he had quite an unsuccessful history with addiction treatment; and she does explore the problems of the demand for abstinence. HOWEVER, she then seems to blame his death completely on the fact that he wasn’t offered a maintenance drug such as buprenorphine or methadone. Here are some excerpts from her article in TheFix:
“Glee” Actor Cory Monteith
Monteith [is a] victim of tough love and… anti-maintenance stigma.
Apparently, these “experts” suggested Eric Clapton’s Crossroads rehab in Antigua, an old-school program that does not “believe in” using medications to treat opioid addiction, despite all the data favoring them as lifesaving for people whose problems involve heroin or painkillers…
We all know what happened next. Although the intervention did get him into treatment… Monteith followed the pattern of the 90% of opioid addicts who are coerced into 12-step recovery and denied an adequate period of maintenance treatment: He relapsed…
Monteith took the deadliest possible combination—alcohol and heroin, whose actions to slow breathing are not additive but multiple—at the deadliest possible time. He was likely not informed about the risk because abstinence-focused rehabs typically don’t provide harm reduction advice. He certainly was not provided with maintenance medication like methadone or buprenorphine that can dramatically reduce that risk; he may not even have know that maintenance was an option…
And this is where stigma, and the fact that addiction medicine generally isn’t practiced like real medicine, take over.
In no other type of treatment are FDA-approved medications seen as appropriate to withhold—without even informing the patient of their existence… If we don’t want to keep losing patients, we’ve got to actually treat addiction like a disease, by providing evidence-based treatment, not just repeating faith-based philosophies.
Denying people access to maintenance care costs lives—and so does failing to provide harm reduction information and tools like naloxone to reverse overdose. The 12 Steps and abstinence are not the only way.
It would seem that she’s obsessed with maintenance drugs like Buprenorphine. With the repeated quotes I bolded above, I don’t know how you could read that article and, regardless of the other content in it, come to any conclusion other than that Monteith died because he wasn’t on Buprenorphine or Methadone. But as she noted, Monteith died of a mixture of alcohol and heroin. He made a deadly mistake. I know people who have made such mistakes. I do not know that Suboxone would’ve stopped them from doing so. I also know people who have simply overdosed on heroin because they made the mistake of using the same extreme amounts of the drug that they used before they became abstinent. Long ago, one of my drug buddies celebrated a year of abstinence from heroin by injecting an entire bundle (ten $10 bags sold on the street) on one occasion. He overdosed and died. It happens. It’s the result of extreme carelessness (or maybe it’s the result of believing that any instance of use will be an extreme instance of use, as has been shown to be the case with alcoholics exposed to AA’s “loss of control/allergy” teachings).
But Maia knows this. She states as much in the article:
…the risk of overdose is highest in the initial few months after being in rehab or any other situation where a period of abstinence has occurred. After a complete detoxification, a person’s tolerance drops precipitously—meaning that the dose they took before treatment without even getting very high may now be potentially fatal. The first two weeks following prison, for example, were shown by one study to carry a greater than 120-fold increased risk of overdose death; that extreme risk elevation holds for whenever the person first uses again after a period without opioids.
But check her last sentence again:
that extreme risk elevation holds for whenever the person first uses again after a period without opioids.
Do maintenance medications actually cause people to stay abstinent? I don’t think so. They are not a panacea. Many people drop off of them, because they simply want to get high (or they use while on them). And, is Maia advocating using them for life? It seems she should, if she thinks that the cause of Monteith’s death is the fact that he wasn’t on a maintenance medication. After all “that extreme risk elevation holds for whenever the person first uses again after a period without opioids.”
Most of the research on drugs like Suboxone (a popular formulation of Buprenorphine and Naloxone) checks the effectiveness of the drug over a 12 week period. That’s it. And as stated above, long term results are essentially unknown. Also, most of the “success” that’s found with drugs like Bupe and Methadone is that people who take it stay engaged in treatment programs longer than those who just receive counseling (without drugs). If the NESARC results from heroin and prescription opiate users are to be factored into the equation, we might decide less treatment is better. After all, those opiate and heroin addicts who received treatment had MUCH longer periods of abuse and dependence before actually remitting. Which in itself means more occasions of use, which means more opportunity to overdose.
The cause of overdose deaths in detoxified opiate users is not a lack of Buprenorphine (or methadone et al) – the cause is the choice to use either a large amount of the drug without having a tolerance that matches the dose – or the choice to mix drugs. Buprenorphine stops physical withdrawal and blocks the high of opiates – both of which contribute to early term “craving.” But why, if someone has already pieced together a substantial amount of time abstinent without a maintenance drug, and thus already dealt with and transcended that early period of “cravings” based on withdrawal, should they then be advised to go on a maintenance drug as our main concern, when the fact is that they could decide to stop taking their buprenorphine at any time, and they will lose their tolerance, and they may choose to get high at any given moment, and still face the same real risk of overdose:they might choose to use the same amount of drug that they used before they lost their tolerance – and die from overdose.
So isn’t this the more important point: if you go abstinent from opiates, you will lose your tolerance to them. Thus, if you then attempt to use opiates again at the same levels you did before you abstained, then you will likely overdose and die.
Shouldn’t we be focused on teaching that point to people? Because regardless of how long they abstain from opiates, they face that risk if they choose to use again. And shouldn’t we also be more focused on fighting the disease message in addiction treatment? That message convinces opiate users that if they make any choice to use substances (including alcohol or marijuana as well) that they will go right back to extreme levels of opiate use. It tells them that their “disease is doing pushups” and that they’ll go right back to the same levels of use, or higher levels, that they had before they became abstinent. It sets up a response expectancy, which is easily much more influential in creating an overdose situation than the lack of a maintenance medication.
Pregnant woman punished for not taking Suboxone
The research shows that people don’t need treatment to get over their addictions – even heroin and other opiate addictions. Yet that doesn’t stop treatment lunatics from forcing it on people – even those who already successfully beat their addictions on their own. As the NYT reports:
She was 14 weeks pregnant and thought she had done the right thing when, at a prenatal checkup, she described a pill addiction the previous year and said she had ended it on her own — something later verified by a urine test. But now an apparently skeptical doctor and a social worker accused her of endangering her unborn child because she had refused to accept their order to start on an anti-addiction drug.
Ms. Beltran thought she was being helpful when, in her first prenatal visit, on July 2, to a clinic at St. Joseph’s Hospital, she discussed her medical history. Ms. Beltran, who worked as a bartender and waitress and became pregnant by a boyfriend who remains close, told the physician assistant that she had become addicted last year to Percocet, a painkiller. But she had willed herself off it the previous fall, even going to the hospital in November for withdrawal symptoms.
She said she was unable to afford a prescription for Suboxone, which blocks other opiates and is widely used in treatment, including during pregnancy. So she obtained some from a friend and, on her own, reduced the dosage over time, stopping altogether three days before her appointment at St. Joseph’s. She said that in May, before she knew she was pregnant, she had taken one Vicodin tablet for a toothache.
The physician assistant, apparently skeptical, said she should get a prescription for Suboxone because withdrawal could be hard on the fetus, Ms. Beltran recalled. “But I told her I’d already tapered off and quit,” she said. A urine test that day found traces of Suboxone but no signs of other opiates, and later tests found her clear of both drugs.
Two weeks after that prenatal visit the social worker showed up unannounced at Ms. Beltran’s home, telling her to restart Suboxone treatment or face a court order to do so. “I told her I’m off this stuff and I don’t want to go back on it,” she recalled, admitting that she lost her temper and shut the door on the social worker after saying, “Maybe I should just get an abortion.”
That’s right – she already quit the drugs, and she even found some Suboxone on the street and used it to detoxify – and stayed clean. She showed desire and initiative before being told what to do. There are countless cases of women citing pregnancy as the reason they chose to quit drugs or alcohol – and successfully doing it, without treatment. Yet with all this, these people still want to force this woman to take Suboxone. She refused, and paid the price:
Two days later, the sheriffs arrived to take her to the county jail and the initial hearing. The case against Ms. Beltran was bolstered by the statement of Dr. Angela Breckenridge, an obstetrician at the West Bend Clinic South at St. Joseph’s Hospital.
In a letter dated July 16, Dr. Breckenridge said that Ms. Beltran had “openly admitted” taking opiates during pregnancy and was still using Suboxone.
“She exhibits lack of self-control and refuses the treatment we have offered her,” wrote Dr. Breckenridge, who, according to Ms. Beltran, had not personally met or examined her. She recommended “a mandatory inpatient drug treatment program or incarceration,” adding, “The child’s life depends on action in this case.”
We know that untreated opiate addicts fare better than treated ones – and here is a case where we’re defying that fact, and forcing someone who already changed on their own – to go into a treatment program which will lower her potential for long term success. And, expecting her to take a drug which may cause complications, as Jacob Sullum noted:
The FDA has assigned buprenorphine to pregnancy category C, meaning “animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks.”
Why would people do this? What is so great about Suboxone? I do not get the obsession with this stuff.
NOTE: I’m not personally against use of drugs such as Buprenorphine or Methadone. If they can help people deal with the tough stage of withdrawal, I’m all for it. I am however skeptical of its use as a “maintenance drug.” But, to each his own. You gotta do what you think is best for you, by your own judgment – so please don’t send me angry emails about my opinion on this matter – I’m not making any recommendation here; I’m not telling anyone to get off such drugs; nor do I don’t think anyone is “bad” or “not really sober” because they use such drugs. I’m simply expressing my confusion as to why they would be so highly recommended when: rates of non-treated recovery are so high; relapse is more common for treated addicts; treatment may exacerbate substance dependence; and the long-term success of these particular treatments is essentially unknown.
I am happy to know some people find these drugs helpful. However, if they are stably abstaining from opiates, then I think they should give THEMSELVES credit for that, rather than giving credit to Suboxone or Methadone. If you wanted to use, you’d just do it; or stop taking Suboxone and do it; or you’d use another drug, like I did when I discovered that injecting cocaine made for a nice high while I was stabilized on methadone. When people truly leave the habit of deriving most of their happiness from chemical highs, they alone are responsible for that choice and change – not a drug.
By Steven Slate
Steven Slate has personally taught hundreds of people how to change their substance use habits through choice - while avoiding the harmful recovery culture and disease model of addiction.
Great article Steven! Of course replacement therapy drug proponents (who coincidentally directly financially benefit from the sale of these drugs) would conclude that Monteith died because he wasn’t taking their drugs. But your argument is absolutely on point – there is no data whatsoever to support that conclusion. Instead there is much data to suggest that Monteith’s death more likely was a result of misinformation he learned in his years in and out of treatment programs; once an addict, always an addict; that he’s powerless over drugs; and that he’ll pick up right where he left off and that he’ll be out of control the moment he picks up again. Yes, that sounds much more plausible.
Since courts uphold that you can’t be sentenced to 12-step treatment, (aging article here http://www.webcitation.org/5lyGIFiqE) I’m a little surprised something similar hasn’t come up to cover this situation. It was my perhaps misguided notion that I can always refuse medical treatment. I find it appalling, and would have loved to see the scene where she tells the social worker “Maybe I should just get an abortion,” followed by a slamming door. Did a court actually enforce her taking the medicine? I’ll try to find out.
Typical government bureaucracy making life changing decisions for other people without, at the very least, common sense. The woman was right in protecting her baby by sharing this info. Had I been the doctor, I would have seen this as her trying to find a healthy way for me to to help her stay on this positive path. I would have thrn set ground rules with her to let her know if she adheres to them we don’t have to go the Suboxone route. If she broke the rules though we would have to use it.
Typical government bureaucracy making life changing decisions for other people without, at the very least, common sense. The woman was right in protecting her baby by sharing this info. Had I been the doctor, I would have seen this as her trying to find a healthy way for me to to help her stay on this positive path & help protect her baby. I would have then set ground rules with her to let her know if she adheres to them we don’t have to go the Suboxone route. If she broke the rules though we would have to use it. In the meantime though we need to set her up with couseling for behavior modification work she can focus on. She clearly was a one-on-one personality. I never understood the insistence of the 12 step program for everybody. If someone is having difficulty already dealing with their own internal stuff, to sit in a room and listen to others internal baggage could be too much for them to handle. One size does not fit all.
This is one of your best in a while, Steven. Excellent stuff.
Suboxone worked well for me. It helped me get off an absolutely insane amount of morphine with vicodin for “breakthrough” pain. I started at 32 mg per day. Now I’m on 2 mg per day. Next month my goal is 1 mg, then half of that, then “half of a half”, until I’m off. I’ll take my time..no need to rush.
It’s madness to force someone to go back on suboxone. It sure helped me, though. A year ago I saw no end to the pain management assembly line. Now I think I really will be free from opiods. Suboxone isn’t a philosopher stone, but it’s a great tool, at leat it’s been that way for me.
is it possible that you’re reversing causation here? perhaps treated user have more problems because their addictions are worse — the reason they seek or receive treatment in the first place.
This site picks and chooses information that backs there argument, don’t be fooled…do your own research. Probably one of the worst sites I’ve come across.
In my experience suboxone is sorta like a stepping stone. I had planned to get high after rehab, long story short I found a sub in my backpack and took that instead. It got rid of all that noise, and made it actually possible to get past those cravings, and reset my focus on recovering. Early recovery is extremely difficult. Early recovery is confusing, it’s full of emotions you haven’t felt in a while, and it’s full of temptation. Simply put suboxone makes everything easier. Taking suboxone alone will not cure the disease of addiction. You can take it every day and still go smoke some crack, or rob the old lady who lives next door to you. The point I’m trying to make is suboxone alone will not get rid of the underlying problems. It won’t get you a job. It won’t stop old habits from resurfacing. It simply eliminates most of the cravings for the day you take it. It allows me to do what is necessary to distance myself from my old self. I’m in a spot where I no longer think of heroin anymore. If I stopped taking the suboxone those feelings and cravings would come back, but nowhere near as strong as the day I got out of rehab. I’m working on myself every day, and everyday is easier and better than the day before. People need to stop with the suboxone shaming, it is an excellent tool to fight this disease. If you don’t agree with maintenance then I’d suggest you don’t use that approach, but as for me I feel that it could help many more people than it already has if doctors explained it is not a cure, but a tool, and if the negative stigmas on it were lifted. Addicts need to stand together. We need to encourage each other and share our experiences and knowledge. I don’t see why it matters if somebody isnt sober while on maintenance. What should matter is if theyre a better person from when they were using, and if they are winning over their addiction. Suboxone is a drug, and I am a drug addict. However, I take it as prescribed, and further myself physically and mentally from the grasp of heroin addiction.
You say you do not understand the idea of Suboxone or Methadone for maintenance. Here it is, if you are diagnosed with a disease by your doctor, you will likely be recommended a medication to start, probably for the rest of your life. Hypertension = blood pressure medications. Diabetes = diabetes medications. High cholesterol = cholesterol medications. So on, so forth. If you are diagnosed with “the disease of addiction” (opioid) you will likely be recommended methadone or Suboxone “for the rest of your life” in order to manage the “disease.”
The disease concept/theory is how medical doctors view any condition or situation. I have even heard that a broken bone is considered an acute “disease,” which can then be treated with medications and surgery.
The problem with the disease model is that it has saturated the addiction treatment setting. It is A concept, not THE concept (as in the only concept).
Your completely off your rocker. Addiction being a choice? Not needing treatment to deal with the underlying issues? Your statistics are bogus. Now meetings and treatment doesn’t work for everyone (mostly those not ready to make changes). You know nothing of the chemistry of the brain and the physical effects of opiods to make any of these claims. Wondering where you received your doctorate in this field, or where your credentials for treatment were gained. This type of misinformation is DANGEOUS and can get people killed. Too bad the 2nd amendment protects even these HORRENDOUS OPINIONS.
The more weapons we have in our arsenal the better, period. I can tell you from my hundreds of terrifying and agonizing withdrawal experiences from opiates that Suboxone is a life saver for me and has much different dynamics on my addiction, I never crave it or abuse it and it works awesome. Know when I was in and out of Methadone clinics for several years it made things worse, it was just like heroine to me I just wanted more and the clinics treated me like a piece of shit even when I was paying them $480 a month, I’ll never forget how terrible the environment you have to subject yourself to at the Methadone clinics every morning. I can’t say Suboxone is better financially it cost $600 a month but you get to take it home and your not treated like a scumbag everyday.
Great article Steven! Of course replacement therapy drug proponents (who coincidentally directly financially benefit from the sale of these drugs) would conclude that Monteith died because he wasn’t taking their drugs. But your argument is absolutely on point – there is no data whatsoever to support that conclusion. Instead there is much data to suggest that Monteith’s death more likely was a result of misinformation he learned in his years in and out of treatment programs; once an addict, always an addict; that he’s powerless over drugs; and that he’ll pick up right where he left off and that he’ll be out of control the moment he picks up again. Yes, that sounds much more plausible.
Since courts uphold that you can’t be sentenced to 12-step treatment, (aging article here http://www.webcitation.org/5lyGIFiqE) I’m a little surprised something similar hasn’t come up to cover this situation. It was my perhaps misguided notion that I can always refuse medical treatment. I find it appalling, and would have loved to see the scene where she tells the social worker “Maybe I should just get an abortion,” followed by a slamming door. Did a court actually enforce her taking the medicine? I’ll try to find out.
Typical government bureaucracy making life changing decisions for other people without, at the very least, common sense. The woman was right in protecting her baby by sharing this info. Had I been the doctor, I would have seen this as her trying to find a healthy way for me to to help her stay on this positive path. I would have thrn set ground rules with her to let her know if she adheres to them we don’t have to go the Suboxone route. If she broke the rules though we would have to use it.
Typical government bureaucracy making life changing decisions for other people without, at the very least, common sense. The woman was right in protecting her baby by sharing this info. Had I been the doctor, I would have seen this as her trying to find a healthy way for me to to help her stay on this positive path & help protect her baby. I would have then set ground rules with her to let her know if she adheres to them we don’t have to go the Suboxone route. If she broke the rules though we would have to use it. In the meantime though we need to set her up with couseling for behavior modification work she can focus on. She clearly was a one-on-one personality. I never understood the insistence of the 12 step program for everybody. If someone is having difficulty already dealing with their own internal stuff, to sit in a room and listen to others internal baggage could be too much for them to handle. One size does not fit all.
This is one of your best in a while, Steven. Excellent stuff.
Suboxone worked well for me. It helped me get off an absolutely insane amount of morphine with vicodin for “breakthrough” pain. I started at 32 mg per day. Now I’m on 2 mg per day. Next month my goal is 1 mg, then half of that, then “half of a half”, until I’m off. I’ll take my time..no need to rush.
It’s madness to force someone to go back on suboxone. It sure helped me, though. A year ago I saw no end to the pain management assembly line. Now I think I really will be free from opiods. Suboxone isn’t a philosopher stone, but it’s a great tool, at leat it’s been that way for me.
is it possible that you’re reversing causation here? perhaps treated user have more problems because their addictions are worse — the reason they seek or receive treatment in the first place.
This site picks and chooses information that backs there argument, don’t be fooled…do your own research. Probably one of the worst sites I’ve come across.
In my experience suboxone is sorta like a stepping stone. I had planned to get high after rehab, long story short I found a sub in my backpack and took that instead. It got rid of all that noise, and made it actually possible to get past those cravings, and reset my focus on recovering. Early recovery is extremely difficult. Early recovery is confusing, it’s full of emotions you haven’t felt in a while, and it’s full of temptation. Simply put suboxone makes everything easier. Taking suboxone alone will not cure the disease of addiction. You can take it every day and still go smoke some crack, or rob the old lady who lives next door to you. The point I’m trying to make is suboxone alone will not get rid of the underlying problems. It won’t get you a job. It won’t stop old habits from resurfacing. It simply eliminates most of the cravings for the day you take it. It allows me to do what is necessary to distance myself from my old self. I’m in a spot where I no longer think of heroin anymore. If I stopped taking the suboxone those feelings and cravings would come back, but nowhere near as strong as the day I got out of rehab. I’m working on myself every day, and everyday is easier and better than the day before. People need to stop with the suboxone shaming, it is an excellent tool to fight this disease. If you don’t agree with maintenance then I’d suggest you don’t use that approach, but as for me I feel that it could help many more people than it already has if doctors explained it is not a cure, but a tool, and if the negative stigmas on it were lifted. Addicts need to stand together. We need to encourage each other and share our experiences and knowledge. I don’t see why it matters if somebody isnt sober while on maintenance. What should matter is if theyre a better person from when they were using, and if they are winning over their addiction. Suboxone is a drug, and I am a drug addict. However, I take it as prescribed, and further myself physically and mentally from the grasp of heroin addiction.
You say you do not understand the idea of Suboxone or Methadone for maintenance. Here it is, if you are diagnosed with a disease by your doctor, you will likely be recommended a medication to start, probably for the rest of your life. Hypertension = blood pressure medications. Diabetes = diabetes medications. High cholesterol = cholesterol medications. So on, so forth. If you are diagnosed with “the disease of addiction” (opioid) you will likely be recommended methadone or Suboxone “for the rest of your life” in order to manage the “disease.”
The disease concept/theory is how medical doctors view any condition or situation. I have even heard that a broken bone is considered an acute “disease,” which can then be treated with medications and surgery.
The problem with the disease model is that it has saturated the addiction treatment setting. It is A concept, not THE concept (as in the only concept).
Your completely off your rocker. Addiction being a choice? Not needing treatment to deal with the underlying issues? Your statistics are bogus. Now meetings and treatment doesn’t work for everyone (mostly those not ready to make changes). You know nothing of the chemistry of the brain and the physical effects of opiods to make any of these claims. Wondering where you received your doctorate in this field, or where your credentials for treatment were gained. This type of misinformation is DANGEOUS and can get people killed. Too bad the 2nd amendment protects even these HORRENDOUS OPINIONS.
The more weapons we have in our arsenal the better, period. I can tell you from my hundreds of terrifying and agonizing withdrawal experiences from opiates that Suboxone is a life saver for me and has much different dynamics on my addiction, I never crave it or abuse it and it works awesome. Know when I was in and out of Methadone clinics for several years it made things worse, it was just like heroine to me I just wanted more and the clinics treated me like a piece of shit even when I was paying them $480 a month, I’ll never forget how terrible the environment you have to subject yourself to at the Methadone clinics every morning. I can’t say Suboxone is better financially it cost $600 a month but you get to take it home and your not treated like a scumbag everyday.