

They’re screaming it from the rooftops: “addiction is a disease, and you can’t stop it without medical treatment”! But why are they screaming it so loud, why are they browbeating us about it, why is it always mentioned with a qualifier? You don’t hear people constantly referring to cancer as “the disease of cancer” – it’s just “cancer”, because it’s obvious that cancer is a disease, it’s been conclusively proven that the symptoms of cancer can’t be directly stopped with mere choices – therefore no qualifier is needed. On the other hand, addiction to drugs and alcohol is not obviously a disease, and to call it such we must either overlook the major gaps in the disease argument, or we must completely redefine the term “disease.” Here we will analyze a few key points and show that what we call addiction doesn’t pass muster as a real disease.
Real Diseases versus The Disease Concept or Theory of Drug Addiction
In a true disease, some part of the body is in a state of abnormal physiological functioning, and this causes the undesirable symptoms. In the case of cancer, it would be mutated cells which we point to as evidence of a physiological abnormality, in diabetes we can point to low insulin production or cells which fail to use insulin properly as the physiological abnormality which create the harmful symptoms. If a person has either of these diseases, they cannot directly choose to stop their symptoms or directly choose to stop the abnormal physiological functioning which creates the symptoms. They can only choose to stop the physiological abnormality indirectly, by the application of medical treatment, and in the case of diabetes, dietetic measures may also indirectly halt the symptoms as well (but such measures are not a cure so much as a lifestyle adjustment necessitated by permanent physiological malfunction).
 In addiction, there is no such physiological malfunction. The best physical evidence put forward by the disease proponents falls totally flat on the measure of representing a physiological malfunction. This evidence is the much touted brain scan[1]. The organization responsible for putting forth these brain scans, the National Institute on Drug Abuse and Addiction (NIDA), defines addiction in this way:
In addiction, there is no such physiological malfunction. The best physical evidence put forward by the disease proponents falls totally flat on the measure of representing a physiological malfunction. This evidence is the much touted brain scan[1]. The organization responsible for putting forth these brain scans, the National Institute on Drug Abuse and Addiction (NIDA), defines addiction in this way:
Addiction is defined as a chronic relapsing brain disease that is characterized by compulsive drug seeking and use, despite harmful consequences. It is considered a brain disease because drugs change the brain – they change it’s structure and how it works. These brain changes can be long lasting, and can lead to the harmful behaviors seen in people who abuse drugs.
The NIDA is stating outright that the reason addiction is considered a disease is because of the brain changes evidenced by the brain scans they show us, and that these changes cause the behavior known as addiction, which they characterize as “compulsive drug seeking and use”. There are three major ways in which this case for the disease model falls apart:
- the changes in the brain which they show us are not abnormal at all
- people change their behavior IN SPITE OF the fact that their brain has changed in response to repeated substance use jump to section
- there is no evidence that the behavior of addicts is compulsive (compulsive meaning involuntary) (point two addresses this, as well as some other research that will be presented) jump to section
This all applies equally to “alcoholism” as well. If you’re looking for information on alcoholism, the same theories and logic discussed here are applicable; wherever you see the term addiction used on this site, it includes alcoholism.
Brain Changes In Addicts Are Not Abnormal, and Do Not Prove The Brain Disease Theory
On the first count – the changes in the brain evidenced by brain scans of heavy substance users (“addicts”) do not represent a malfunctioning brain. They are quite normal, as research into neuroplasticity has shown us. Whenever we practice doing or thinking anything enough, the brain changes – different regions and neuronal pathways are grown or strengthened, and new connections are made; various areas of the brain become more or less active depending upon how much you use them, and this becomes the norm in your brain – but it changes again as you adjust how much you use those brain regions depending on what you choose to think and do. This is a process which continues throughout life, there is nothing abnormal about it. Here, Sharon Begley describes neuroplasticity: [2]
The term refers to the brain’s recently discovered ability to change its structure and function, in particular by expanding or strengthening circuits that are used and by shrinking or weakening those that are rarely engaged. In its short history, the science of neuroplasticity has mostly documented brain changes that reflect physical experience and input from the outside world.
So, when the NIDA’s Nora Volkow and others show us changes in the brain of a substance user as compared to a non-substance user, this difference is not as novel as they make it out to be. They are showing us routine neuroplastic changes which every healthily functioning person’s brain goes through naturally. The phenomenon of brain changes isn’t isolated to “addicts” or anyone else with a so-called brain disease – non-addicted and non-depressed and non-[insert brain disease of the week here] people experience neural adaptations too. One poignant example was found in the brains of London taxi drivers, as Begley and Jeffrey Schwartz pointed out in The Mind and The Brain. [4]
Is Being A Good Taxi Driver A Disease?
A specific area of the brain’s hippocampus is associated with creating directional memories and a mental map of the environment. A team of researchers scanned the brains of London taxi drivers and compared their brains to non-taxi drivers. There was a very noticeable difference, not only between the drivers and non-drivers, but also between the more experienced and less experienced drivers:
There it was: the more years a man had been a taxi driver, the smaller the front of his hippocampus and the larger the posterior. “Length of time spent as a taxi driver correlated positively with volume in…the right posterior hippocampus,” found the scientists. Acquiring navigational skills causes a “redistribution of gray matter in the hippocampus” as a driver’s mental map of London grows larger and more detailed with experience. [4]
So, the longer you drive a cab in London (that is, the longer you exert the mental and physical effort to quickly find your way around one of the world’s toughest to navigate cities), the more your brain physically changes. And the longer you use drugs, the more your brain changes. And indeed, the longer and more intensely you apply yourself to any skill, thought, or activity – the more it will change your brain, and the more visible will be the differences between your brain and that of someone who hasn’t been focused on that particular skill. So, if we follow the logic of the NIDA, then London’s taxi drivers have a disease, which we’ll call taxi-ism, that forces them to drive taxis. But the new diseases wouldn’t stop there.
Learning to play the piano well will change your brain – and if you were to compare brain scans of a piano player to a non-piano player, you would find significant differences. Does this mean that piano playing is a disease called Pianoism? Learning a new language changes your brain, are bilingual people diseased? Athletes’ brains will change as a result of intensive practice – is playing tennis a disease? Are soccer players unable to walk into a sporting goods store without kicking every ball in sight? We could go on and on with examples, but the point is this – when you practice something, you get better at doing it, because your brain changes physiologically – and this is a normal process. If someone dedicated a large portion of their life to seeking and using drugs, and their brain didn’t change – then that would be a true abnormality. Something would be seriously wrong with their brain.
Its not just physical activity that changes our brains, thoughts alone can have a huge effect. What’s more, whether the brain changes or not, there is much research which shows that the brain is slave to the mind. As Begley points out elsewhere, thoughts alone can create the same brain activity that would come about by doing things[2]:
Using the brain scan called functional magnetic resonance imaging, the scientists pinpointed regions that were active during compassion meditation. In almost every case, the enhanced activity was greater in the monks’ brains than the novices’. Activity in the left prefrontal cortex (the seat of positive emotions such as happiness) swamped activity in the right prefrontal (site of negative emotions and anxiety), something never before seen from purely mental activity. A sprawling circuit that switches on at the sight of suffering also showed greater activity in the monks. So did regions responsible for planned movement, as if the monks’ brains were itching to go to the aid of those in distress.
So by simply practicing thinking about compassion, these monks made lasting changes in their brain activity. Purely mental activity can change the brain in physiologically significant ways. And to back up this fact we look again to the work of Dr Jeffrey Schwartz[3], who has taught OCD patients techniques to think their way out of obsessive thoughts. After exercising these thought practices, research showed that the brains of OCD patients looked no different than the brains of those who’d never had OCD. If you change your thoughts, you change your brain physically – and this is voluntary. This is outside the realm of disease, this shows a brain which changes as a matter of normality, and can change again, depending on what we practice choosing to think. There is nothing abnormal about a changing brain, and the type of changes we’re discussing aren’t necessarily permanent, as they are characterized to be in the brain disease model of addiction.
These brain change don’t need to be brought on by exposure to chemicals. Thoughts alone, are enough to rewire the very circuits of the human brain responsible for reward and other positive emotions that substance use and other supposedly “addictive” behaviors (“process addictions” such as sex, gambling, and shopping, etc.) are connected with.
The Stolen Concept of Neuroplasticity in the Brain Disease Model of Addiction
Those who claim that addiction is a brain disease readily admit that the brain changes in evidence are arrived at through repeated choices to use substances and focus on using substances. In this way, they are saying the disease is a product of routine neuroplastic processes. Then they go on to claim that such brain changes either can’t be remedied, or can only be remedied by outside means (medical treatment). When we break this down and look at it step by step, we see that the brain disease model rests on an argument similar to the “stolen concept”. A stolen concept argument is one in which the argument denies a fact on which it simultaneously rests. For example, the philosophical assertion that “reality is unknowable” rests on, or presumes that the speaker could know a fact of reality, it presumes that one could know that reality is unknowable – which of course one couldn’t, if reality truly was unknowable – so the statement “reality is unknowable” invalidates itself. Likewise, the brain disease proponents are essentially saying “neuroplastic processes create a state called addiction which cannot be changed by thoughts and choices” – this however is to some degree self-invalidating, because it depends on neuroplasticity while seeking to invalidate it. If neuroplasticity is involved, and is a valid explanation for how to become addicted, then we can’t act is if the same process doesn’t exist when it’s time to focus on getting un-addicted. That is, if the brain can be changed into the addicted state by thoughts and choices, then it can be further changed or changed back by thoughts and choices. Conditions which can be remedied by freely chosen thoughts and behaviors, don’t fit into the general understanding of disease. Ultimately, if addiction is a disease, then it’s a disease so fundamentally different than any other that it should probably have a completely different name that doesn’t imply all the things contained in the term “disease” – such as the idea that the “will” of the afflicted is irrelevant to whether the condition continues.
People change their addictive behavior in spite of the fact that their brain is changed – and they do so without medication or surgery (added 4/18/14)
In the discussion above, we looked at some analogous cases of brain changes to see just how routine and normal (i.e. not a physiological malfunction) such changes are. Now we’re going to look directly at the most popular neuroscientific research which purports to prove that these brain changes actually cause “uncontrolled” substance use (“addiction”).
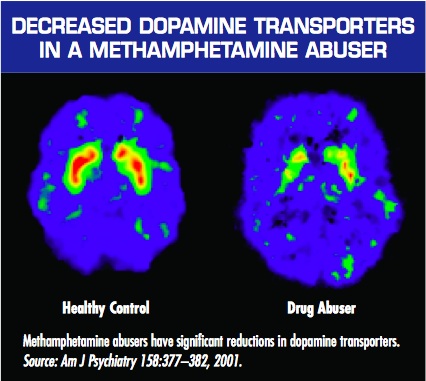
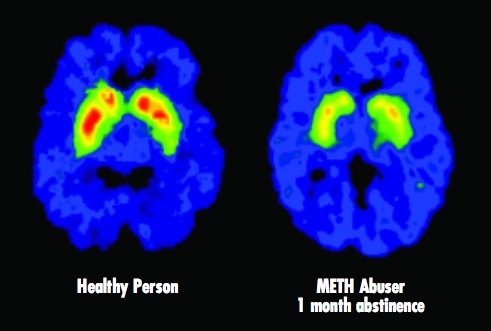
The most popular research is Nora Volkow’s brain scans of “meth addicts” presented by the NIDA. The logic is simple. We’re presented with the brain scan of a meth addict alongside the brain scan of a non-user, and we’re told that the decreased activity in the brain of the meth user (the lack of red in the “Drug Abuser” brain scan presented) is the cause of their “compulsive” methamphetamine use. Here’s how the National Institute on Drug Abuse (NIDA) explains the significance of these images in their booklet – Drugs, Brains, and Behavior: The Science of Addiction :
Just as we turn down the volume on a radio that is too loud, the brain adjusts to the overwhelming surges in dopamine (and other neurotransmitters) by producing less dopamine or by reducing the number of receptors that can receive signals. As a result, dopamine’s impact on the reward circuit of a drug abuser’s brain can become abnormally low, and the ability to experience any pleasure is reduced. This is why the abuser eventually feels flat, lifeless, and depressed, and is unable to enjoy things that previously brought them pleasure. Now, they need to take drugs just to try and bring their dopamine function back up to normal.
[emphasis added]
They go on that these same sorts of brain changes:
..may also lead to addiction, which can drive an abuser to seek out and take drugs compulsively. Drug addiction erodes a person’s self-control and ability to make sound decisions, while sending intense impulses to take drugs.
[emphasis added]
That image is shown when NIDA is vaguely explaining how brain changes are responsible for “addiction.” But later on, when they try to make a case for treating addiction as a brain disease, they show the following image, which tells a far different story if you understand more of the context than they choose to mention:
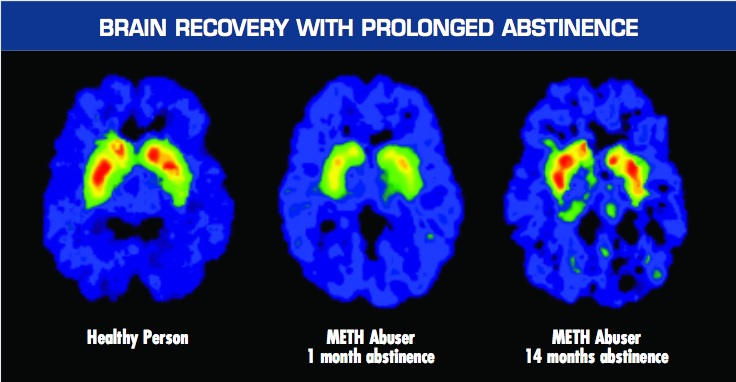
Again, this graphic is used to support the idea that we should treat addiction as a brain disease. However, the authors mistakenly let a big cat out of the bag with this one – because the brain wasn’t treated at all. Notice how the third image shows a brain in which the red level of activity has returned almost to normal after 14 months of abstinence. That’s wonderful – but it also means that the NIDA’s assertions that “Addiction means being unable to quit, even in the face of negative consequences”(LINK) and “It is considered a brain disease because drugs change the brain… These brain changes… can lead to the harmful behaviors seen in people who abuse drugs” are dead wrong.
When these studies were done, nobody was directly treating the brain of methamphetamine addicts. They were not giving them medication for it (there is no equivalent of methadone for speed users), and they weren’t sticking scalpels into the brains of these meth addicts, nor were they giving them shock treatment. So what did they do?
These methamphetamine addicts were court ordered into a treatment program (whose methodology wasn’t disclosed in the research) which likely consisted of a general mixture of group and individual counseling with 12-step meeting attendance. I can’t stress the significance of this enough: their brains were not medically treated. They talked to counselors. They faced a choice between jail and abstinence. They CHOSE abstinence (for at least 14 months!) – even while their brains had been changed in a way that we’re told robs them of the ability to choose to quit “even in the face of negative consequences.” [5]
Even with changed brains, people are capable of choosing to change their substance use habits. They choose to stop using drugs, and as the brain scans above demonstrate – their brain activity follows this choice. If the brain changes caused the substance using behavior, i.e. if it was the other way around, then a true medical intervention should have been needed – the brain would’ve needed to have changed first via external force (medicine or surgery) before abstinence was initiated. They literally wouldn’t have been able to stop for 14 months without a real physical/biological medical intervention. But they did…
Substance Use Is Not Compulsive, It Is A Choice
In his classic book Addiction & Opiates, Alfred R Lindesmith PhD explained the requirements of reliable scientific theories explaining the causes of things such as heroin addiction:
…a genuine theory that proposes to explain a given phenomenon by relating it to another phenomenon must, in the first place, have clear empirical implications which, if not fulfilled, negate the theory.
If the theory is that neural adaptations alone cause uncontrolled behavior, then this proposition can easily be shown to be false. I demonstrated above that in the midst of having fully “changed” or “addicted” brains, people do indeed stop using substances, so essentially, it is case closed. But the depths to which the brain disease theory of addiction can be negated go even further, because the basic theory of addiction as representing uncontrolled substance use has never been explained. Explanation of the mechanism by which substance use happens without the individual’s consent is conspicuously missing – yet such explanation is a necessary part of such a theory, as Lindesmith writes (again in Addiction & Opiates):
…besides identifying the two types of phenomenon that are allegedly interrelated, there must be a description of the processes or events that link them. In other words, besides affirming that something causes something else, it is necessary to indicate how the cause operates to produce the alleged effect.
“Here Comes the Bogey-Man” by Goya, circa 1799
There doesn’t seem to be any explanation or evidence that substance use is involuntary. In fact, the evidence, such as that presented above, shows the opposite. Nevertheless, when the case for the disease is presented, the idea that drug use is involuntary is taken for granted as true. No evidence is ever actually presented to support this premise, so there isn’t much to be knocked down here, except to make the point I made above – is a piano player fundamentally incapable of resisting playing the piano? They may love to play the piano, and want to do it often, they may even be obsessive about it, but it would be hard to say that at the sight of a piano they are involuntarily driven by their brain to push aside whatever else they need to do in order to play that piano.
There is another approach to the second claim though. We can look at the people who have subjectively claimed that their substance use is involuntary, and see if the offer of incentives results in changed behavior. Gene Heyman covered this in his landmark book, Addiction: A Disorder of Choice[3]. He recounts studies in which cocaine abusers were given traditional addiction counseling, and also offered vouchers which they could trade in for modest rewards such as movie tickets or sports equipment – if they proved through urine tests that they were abstaining from drug use. In the early stages of the study, 70% of those in the voucher program remained abstinent, while only 20% stayed abstinent in the control group which didn’t receive the incentive of the vouchers. This demonstrates that substance use is not in fact compulsive or involuntary, but that it is a matter of choice, because these “addicts” when presented with a clear and immediately rewarding alternative to substance use and incentive not to use, chose it. Furthermore, follow up studies showed that this led to long term changes. A full year after the program, the voucher group had double the success rate of those who received only counseling (80% to 40%, respectively). This ties back in to our first point that what you practice, you become good at. The cocaine abusers in the voucher group practiced replacing substance use with other activities, such as using the sports equipment or movie passes they gained as a direct consequence of abstaining from drug use – thus they made it a habit to find other ways of amusing themselves, this probably led to brain changes, and the new habits became the norm.
Long story short, there is no evidence presented to prove that substance use is compulsive. The only thing ever offered is subjective reports from drug users themselves that they “can’t stop”, and proclamations from treatment professionals that the behavior is compulsive due to brain changes. But if the promise of a ticket to the movies is enough to double the success rate of conventional addiction counseling, then it’s hard to say that substance users can’t control themselves. The reality is that they can control themselves, but they just happen to see substance use as the best option for happiness available to them at the times when they’re abusing substances. When they can see other options for happiness as more attractive (i.e. as promising a greater reward than substance use), attainable to them, and as taking an amount of effort they’re willing to expend – then they will absolutely choose those options instead of substance use, and will not struggle to “stay sober”, prevent relapse, practice self-control or self-regulation, or any other colloquialism for making a different choice. They will simply choose differently.
But wait… there’s more! (Added 4/21/14) Contrary to the claims that alcoholics and drug addicts literally lose control of their substance use, a great number of experiments have found that they are really in full control of themselves. Priming dose experiments have found that alcoholics are not triggered into uncontrollable craving after taking a drink. Here’s a link to the evidence and a deeper discussion of these findings: Do Addicts and Alcoholics Lose Control? Priming dose experiments of cocaine, crack, and methamphetamine users found that after being given a hit of their drug of choice (primed with a dose) they are capable of choosing a delayed reward rather than another hit of the drug.
Three Most Relevant Reasons Addiction Is Not A Disease
So to sum up, there are at least two significant reasons why the current brain disease theory of addiction is false.
- A disease involves physiological malfunction, the “proof” of brain changes shows no malfunction of the brain. These changes are indeed a normal part of how the brain works – not only in substance use, but in anything that we practice doing or thinking intensively. Brain changes occur as a matter of everyday life; the brain can be changed by the choice to think or behave differently; and the type of changes we’re talking about are not permanent.
- The very evidence used to demonstrate that addicts’ behavior is caused by brain changes also demonstrates that they change their behavior while their brain is changed, without a real medical intervention such as medication targeting the brain or surgical intervention in the brain – and that their brain changes back to normal AFTER they VOLITIONALLY change their behavior for a prolonged period of time
- Drug use in “addicts” is not compulsive. If it was truly compulsive, then offering a drug user tickets to the movies would not make a difference in whether they use or not – because this is an offer of a choice. Research shows that the offer of this choice leads to cessation of substance abuse. Furthermore, to clarify the point, if you offered a cancer patient movie tickets as a reward for ceasing to have a tumor – it would make no difference, it would not change his probability of recovery.
Addiction is NOT a disease, and it matters. This has huge implications for anyone struggling with a substance use habit.
References:
- 1) NIDA, Drugs Brains and Behavior: The Science of Addiction, sciofaddiction.pdf
- 2) Sharon Begley, Scans of Monks’ Brains Show Meditation Alters Structure, Functioning, Wall Street Journal, November 5, 2004; Page B1, http://psyphz.psych.wisc.edu/web/News/Meditation_Alters_Brain_WSJ_11-04.htm
- 3) Gene Heyman, Addiction: A Disorder of Choice, Harvard University Press, 2009
- 4) Sharon Begley and Jeffrey Schwartz, The Mind And The Brain, Harper Collins, 2002
- 5) Links to the 2 methamphetamine abuser studies by Nora Volkow:
http://www.jneurosci.org/cgi/content/full/21/23/9414
http://ajp.psychiatryonline.org/cgi/reprint/158/3/377
Important Notes from the author to readers and especially commenters:
On “badness” or immorality:
Please do not attribute to me the idea that heavy substance users must be “bad” or “immoral” if they are in fact in control of and choosing their behavior. I do not think this. I think that at the time they’re using, it is what they prefer, given what life options they believe are available to them – and I don’t think it’s my job to decide what other people should prefer for themselves, and then declare them bad if they don’t live up to my vision of a “good” life. That’s what the disease recovery culture does, de facto, when they present the false dichotomy of ‘diseased or bad’. To say that addiction is chosen behavior is simply to make a statement about whether the behavior is within the control of the individual – it is not a judgment of the morality of the behavior or the individual choosing it.
On willpower:
Please do not attribute to me the suggestion to “use willpower.” I have not said that people should use willpower, nor do I think it’s a coherent or relevant concept in any way, nor do I think “addicts lack willpower” or that those who recover have more willpower, nor, and this is important, do I believe that a choice model of addiction necessarily implies willpower as the solution.
“Addicts” do not need extra willpower, strength, or support, to change their heavy substance use habits if that is what they want to do. They need to change their preference for heavy substance use, rather than trying to fight that preference with supposed “willpower.”
On compassion:
Please don’t accuse me of not having compassion for people who have substance use problems. You do not know that, and if you attack my motives in this way it just shows your own intellectual impotence and sleaze. I have a great deal of compassion for people with these problems – I was once one such person. I am trying to get at the truth of the nature of addiction, so that the most people can be helped in the most effective way possible. I don’t doubt the compassion of those who believe addiction is a disease, and I hope you’ll give me the same benefit of the doubt. I assure you I care and want the best for people – and I don’t need to see them as diseased to do so. When you see someone who’s gotten themselves into a mess, don’t you want to help, even if it’s of their own making? Why should we need to believe they have a disease to help them if the mess is substance use related? I don’t get that requirement.
Some Agreement I’ve Found From Addiction Researchers (added 6/10/14)
I began working out my understanding of the brain disease model back in 2005 as I started working on a book about addiction; published this article in 2010; and was happy to find in 2011 when I went back to work with Baldwin Research that they had arrived at a similar conclusion. The way they stated it amounted to “either everything is addiction, or nothing is” – referring to the fact that the brain changes presented as proof of addiction being a brain disease are so routine as to indicate that all behavior must be classified as addiction if we follow the logic.
I was also gratified to have found a neuroscientist who arrived at the same conclusions. I think Marc Lewis PhD and I may disagree on a few things, but it seems we may see eye to eye on the logic I presented above about such brain changes being routine, and thus not indicative of disease. Check what he wrote in 2012 for the PLOS Blog, Mind The Brain:
every experience that has potent emotional content changes the NAC and its uptake of dopamine. Yet we wouldn’t want to call the excitement you get from the love of your life, or your fifth visit to Paris, a disease. The NAC is highly plastic. It has to be, so that we can pursue different rewards as we develop, right through childhood to the rest of the lifespan. In fact, each highly rewarding experience builds its own network of synapses in and around the NAC, and that network sends a signal to the midbrain: I’m anticipating x, so send up some dopamine, right now! That’s the case with romantic love, Paris, and heroin. During and after each of these experiences, that network of synapses gets strengthened: so the “specialization” of dopamine uptake is further increased. London just doesn’t do it for you anymore. It’s got to be Paris. Pot, wine, music…they don’t turn your crank so much; but cocaine sure does. Physical changes in the brain are its only way to learn, to remember, and to develop. But we wouldn’t want to call learning a disease.
….
In my view, addiction (whether to drugs, food, gambling, or whatever) doesn’t fit a specific physiological category. Rather, I see addiction as an extreme form of normality, if one can say such a thing. Perhaps more precisely: an extreme form of learning. No doubt addiction is a frightening, often horrible, state to endure, whether in oneself or in one’s loved ones. But that doesn’t make it a disease.
I think that quote is very important, because it highlights neuronal changes that occur in the same region implicated in addiction (whereas the examples I presented earlier in the article represented some other regions).
In a brilliant paper titled “The naked empress: Modern neuro science and the concept of addiction”, Peter Cohen of The Centre for Drug Research at University of Amsterdam, states that:
The notions of addiction transformed into the language of neurology as performed by authors like Volkov, Berridge, Gessa or De Vries are completely tautological.
He essentially argues that Volkow et al take for granted that heavy drug and alcohol use is uncontrolled, identify neural correlates, and present them as evidence of uncontrollability. Yet they don’t do so with other behaviors, and he provides plenty of examples. He notes that they start with assumptions that certain patterns of behavior (e.g. heavy drug use) are uncontrolled, and others are controlled – based purely on cultural prejudices. He accurately identifies addiction as a learned behavior, or as routine bonding to a thing, and then expresses something very close to my thesis presented above (that all learned/intensely repeated behaviors result in “brain changes”).
The problem of course is that probably all learning produces temporary or lasting ‘change in neural systems’. Also, continuation of learned behavior may be functional in the eyes and experience of the person but less so in the eyes of the outsider. Who is right? We know of people remaining married in spite of-in the eyes of a beholder- a very bad marriage. Who speaks of lasting ‘neural change’ as the basis of the continued marriage? But, even when a person herself sees some behavior as counter functional, it is not necessarily seen as addiction. It may be seen as impotence, ingrained habit or unhappy adaptation. It all depends on which behavior we discuss, not on the brain.
The great points contained in this article would be done an injustice if I tried to sum them up here, so check it out for yourself at The Center for Drug Research University of Amsterdam. As with Marc Lewis, I suspect that Peter Cohen and I might have some substantial disagreements about the full nature of addiction and human behavior in general, but I think we at least agree that the changes in the brain of an “addict” do not necessarily represent disease, and more likely represent a routine process.
Writing in 2013 for the journal Frontiers In Psychiatry, esteemed behavioral and addiction researcher Gene Heyman pointed out something so painfully obvious that we don’t even take notice – no causal link has ever been found between the neural adaptations caused by excessive substance use and continued heavy use. That is, correlation is not causation:
With the exception of alcohol, addictive drugs produce their biological and psychological changes by binding to specific receptor sites throughout the body. As self-administered drug doses greatly exceed the circulating levels of their natural analogs, persistent heavy drug use leads to structural and functional changes in the nervous system. It is widely – if not universally – assumed that these neural adaptations play a causal role in addiction. In support of this interpretation brain imaging studies often reveal differences between the brains of addicts and comparison groups (e.g., Volkow et al., 1997; Martin-Soelch et al., 2001) However, these studies are cross-sectional and the results are correlations. There are no published studies that establish a causal link between drug-induced neural adaptations and compulsive drug use or even a correlation between drug-induced neural changes and an increase in preference for an addictive drug.
Did you get that? Let me repeat the words of this experienced researcher, PhD, and lecturer/professor from Boston College and Harvard who, in addition to publishing scores of papers in peer reviewed medical journals has also had an entire book debunking the disease model of addiction by Harvard University press (I say all of this about his credentials so that I can hopefully STOP getting commenters who say “but you’re not a doctor, and what are your credentials wah, wah, wah,……” here’s a “credentialed” expert who essentially agrees with most of what I’ve written in this article – so please, for the love of god, save your fallacious ad hominems and appeals to authority for another day!)- he (Gene Heyman PhD) said this, as of 2013:
There are no published studies that establish a causal link between drug-induced neural adaptations and compulsive drug use or even a correlation between drug-induced neural changes and an increase in preference for an addictive drug.
And this was in a recently published paper in a section headed “But Drugs Change the Brain”, in which he continued to debunk the “brain changes cause addiction” argument by saying:
There are no published studies that establish a causal link between drug-induced neural adaptations and compulsive drug use or even a correlation between drug-induced neural changes and an increase in preference for an addictive drug. For example, in a frequently referred to animal study, Robinson et al. (2001) found dendritic changes in the striatum and the prefrontal cortex of rats who had self-administered cocaine. They concluded that this was a “recipe for addiction.” However, they did not evaluate whether their findings with rodents applied to humans, nor did they even test if the dendritic modifications had anything to do with changes in preference for cocaine in their rats. In principle then it is possible that the drug-induced neural changes play little or no role in the persistence of drug use. This is a testable hypothesis.
First, most addicts quit. Thus, drug-induced neural plasticity does not prevent quitting. Second, in follow-up studies, which tested Robinson et al.’s claims, there were no increases in preference for cocaine. For instance in a preference test that provided both cocaine and saccharin, rats preferred saccharin (Lenoir et al., 2007) even after they had consumed about three to four times more cocaine than the rats in the Robinson et al study, and even though the cocaine had induced motoric changes which have been interpreted as signs of the neural underpinnings of addiction (e.g., Robinson and Berridge, 2003). Third [an analysis of epidemiological studies] shows that the likelihood of remission was constant over time since the onset of dependence. Although this is a surprising result, it is not without precedent. In a longitudinal study of heroin addicts, Vaillant (1973) reports that the likelihood of going off drugs neither increased nor decreased over time (1973), and in a study with rats, Serge Ahmed and his colleagues (Cantin et al., 2010) report that the probability of switching from cocaine to saccharin (which was about 0.85) was independent of past cocaine consumption. Since drugs change the brain, these results suggest that the changes do not prevent quitting, and the slope of [an analysis of epidemiological studies] implies that drug-induced neural changes do not even decrease the likelihood of quitting drugs once dependence is in place.
Read the full paper here – it’s an amazingly concise summary of the truths about addiction that contradict many of the accepted opinions pushed by the recovery culture – Heyman, G. M. (2013). Addiction and Choice: Theory and New Data. Frontiers in Psychiatry, 4. doi:10.3389/fpsyt.2013.00031
Why Does It Matter Whether or Not Addiction Is A Brain Disease?
When we accept the unproven view that addiction and alcoholism are brain diseases, then it will lead us down a long, painful, costly, and pointless road of cycling in and out of ineffective treatment programs and 12 step meetings. You will waste a lot of time without finding a permanent solution. When we examine the evidence, throw out the false disease concepts, and think rationally about the problem we can see that addiction is really just a matter of choice. Knowing this, we can bypass the rehabs, and find the true solution within ourselves. You can choose to end your addiction. You can choose to improv your life. You can choose to stop the endless cycle of “recovery” and start living. You don’t need to be a victim of the self-fulfilling prophecy that is the brain disease model of addiction. There are alternative views and methods of change which I hope you’ll take the time to learn about on The Clean Slate Addiction Site.
There are many different ways to argue against the brain disease model of addiction. I have only presented 3 basic arguments here. But beyond just addiction, many modern claims of “brain disease” are fatally flawed, in that they are founded on the logically impossible philosophical stance of psychological determinism. From this standpoint, any evidence of any brain activity is immediately interpreted as a “cause” of a particular mind state or behavior – with no regard for free will/the ability to choose one’s thoughts and thus behaviors. If you understand the impossibility of psychological determinism (or “epiphenomenalism”) then you’ll take all such claims with a grain of salt. For a detailed examination of this issue, see the following article: The Philosophical Problem with the Brain Disease Model of Addiction: Epiphenomenalism
How To End Addiction, Substance Dependence, Substance Abuse, Alcoholism, and General Drug and Alcohol Problems (updated 11/4/2015)
Due to the fact that most conventional rehab and addiction treatment programs follow the false belief that addiction is a disease, they are generally not effective at dealing with these problems – so I really can’t ethically recommend any “treatment” programs other than a run of the mill detoxification procedure if you feel you may be experiencing physical withdrawal symptoms – you can find that through your local hospital or emergency room; by asking your primary care doctor; or by calling 911 if you feel your life is in danger due to withdrawal (beware that withdrawal from alcohol and some prescription drugs such as the class known as benzodiazepines can lead to fatal seizures). But what comes after detoxification is simply personal choices, and treatment programs actually discourage productive personal choices by attempting to control people and feeding them nonsense such as the disease theory and idea of powerlessness.
If you want to end or alter your own substance use habits you need to make the choice to do so. Many readers will object to this answer as flippant, cruel, out of touch, et cetera. I realize this, but I chose to change, and in reality everyone who moves beyond problematic substance use chooses to change as well.
There is too much to unpack within what people believe is contained in the statement “choose to change.” I have tried to address some of that here in the past, but I realize this article is not the place to do that. This article’s scope needs to remain limited to the question of whether or not addiction is a disease.
My conclusion is that addiction is freely chosen behavior, and that the person who continues heavy substance use despite mounting costs still sees heavy substance use as their best viable option at the time they’re doing it – even though they recognize many costs and downsides. Choosing to change then, really means that they rethink whether heavy substance use is their best viable option. The only way I know to come to new conclusions is to re-examine the issues methodically, and this may often mean gathering new information and perspectives. Thus, the help that can be given to troubled heavy substance users is information. Helpers can provide accurate information that troubled people can use to change their perspective and come to believe they have better viable options than continued heavy problematic substance use.
I endeavor to give accurate information here that will help people to understand that change is possible, and that they are not doomed to a lifetime of addiction. Hopefully, this helps them on their way to believing in better viable options.
About this article:
I originally published this article on September 25, 2010. I have since added some significant supporting work I was able to find over the years, and those additions are noted. Some other minor edits from the original article are not noted.
Author
Hi, I’m, Steven Slate, the author of this post and of all content on this website. Yes, I was what you would call an “addict.” If you want to know more about me, go to the About page. If you want quotes from PhDs and such (as if I haven’t given enough here already) go to my Quotes From Experts About Addiction page. Please be civil in your comments, and many of your angry comments may already be answered on my FAQs page, so maybe check that out before you scream at me.
I’m an addict and this article makes way more sense to me than someone trying to tell me I have no control over my behavior and that I’m powerless. that’s just bullshit and the idea that I have no control is harmful to my ability to actually make lasting changes to my behavior. the disease theory is bullshit and rehabs love to use it cause it keep addicts coming back and paying for treatment that for most people doesn’t help them at all.
i agree with the first comment made. I feel exactly the same way
I always knew I didn’t have a disease. I always say in the AA meetings, if being a human being is a disease, than I am a disease, but that’s not true, I don’t have a disease,. I am just a human being
thank you so much for the info
I copy and pasted it and will read most of it to people when I am a speaker at an AA meeting even though I know they will bicker about it and put me down in cross talk which will just make me feel sorry for them
That’s what you’re gonna do? You’re going to take over your meeting and push that on people? Either go to 12 step meetings or don’t, but if you’re going to disrespect the traditions and inappropriately share that as a SPEAKER, why not just stop going? Whether the article/your views are right or not, there’s a time and a place, and that’s not it.
I don’t understand this at all. I didn’t choose to become addicted to methamphetamine, I didn’t choose to hurt everyone around me by using drugs. I tried my hardest to get away from such substances. Not once did I ever choose to become the person I had become. Yes, people f*** up, but my no means does that mean they’re consciously making the decision to become a drug addict or an alcoholic. I chose to get clean. That was where I said enough was enough. Nobody chooses to hurt those who they love and those who love them. I’m not entirely sure you know what being a drug addict is all about.
I didn’t choose to get caught up with the law. I wasn’t given a choice in whether or not my best friend overdosed in front of me and ended up in the hospital. If I had the choice beforehand, I wouldn’t ever have touched the crap! So please understand things before you post about them.
Katie,
Unless you were unfortunately and physically FORCED to take illegal drugs each and every time you took them, your comment sounds as though you want people to believe you had NOTHING to do with obtaining and using the drug of your choice.
Assuming you were NOT forced, YOU (NOBODY ELSE) had to make the conscious decision and choice to use drugs EACH and EVERY time YOU used them. You want everyone (except you) to believe you have no fault…it’s always someone else’s fault. You wrote, “I didn’t choose to become addicted to methamphetamine”. By choosing to use too much, too often, YOU (NOBODY ELSE) caused your body to become dependent on the drug. So, yes YOU did choose to become addicted by not saying a simple two-letter word right from the beginning…NO!!!!!!!!!
You did not want to hurt anyone nor did you want to become the person you had become but those were some of the consequences of YOUR CHOICE to take drugs. You also wrote, “…but by no means does that mean they’re consciously making the decision to become a drug addict or an alcoholic”. Not true…anybody who uses, in excess, is a potential addict.
You also wrote, “I didn’t choose to get caught up with the law.” WRONG, again!! Every time YOU chose to use drugs, YOU gave the law another invitation to arrest and prosecute you. You also wrote, “I wasn’t given a choice in whether or not my best friend overdosed in front of me and ended up in the hospital.” You ARE partially correct…using was HER choice, you being with her was YOUR choice. You also wrote, “If I had the choice beforehand, I wouldn’t ever have touched the crap!” As I have written already, YOU DID have the choice beforehand…EVERY time you used.
The best choice you have made since your ordeal started was to get clean!!!! I hope you stay clean and have a happy life!!!!
If a person believes it is a disease or not a disease, what does it matter to anyone? The point is that person is willing to stop – It gets me when people criticize other people who get sober on their own, through a church, 12-step program, or some other way. Yes, I am an AA member, but I also believe it does not matter which way any person goes only that he/she is improving their life.
So your opinion is that people’s beliefs do not influence their actions?
If that is so, then why are you trying to convince anyone to believe that the belief in the disease model of addiction doesn’t matter? If it doesn’t matter then it doesn’t matter and the very act of you typing your comments here was a completely futile, nihilistic waste of time and your own existence on this planet.
This just seems mean. The person is trying to say they appreciate a person’s motives over their thinking process, and you bring it into somehow proving their “waste of existence”?
This shows the hidden anger (who knows at what?) you don’t show in your well-worded post about the disease model debate, or you’d have seen this commenter’s response as among the least objectionable.
Read your response again vs Maira’s and see how you warped a nice latitudinarian sentiment into a pseudophilosophical insult. It helped me see that your motives are from anger, not to help others. Are you against people improving their lives?
I hope it doesn’t appear that I have hidden anger. I have open, admitted anger over such comments. They are among the most infuriating comments I get here. Hers is not the worst, but it’s a constant theme – “who cares if it’s a disease” – well now I answered all who say that above. I appreciate those who put forward a poorly reasoned defense of the disease model more than those who come here to say “who cares.”
As for motives, I’m not sure why you are attacking mine -I won’t speculate on yours. I will defend myself though. I am not walking into an AA meeting or a rehab and telling everyone that they’re jerks for believing that addiction is a disease. Nor does my article read as such. I believe that your beliefs affect your behavior. The disease proponents also inherently believe the same, as evidenced by the fact that they make it their mission to spread the idea that addiction is a disease, and they make it top priority to “admit that you have a disease” (or that you are powerless, which is essentially the same) if you are to make any progress in dealing with your substance use problem. They will not stop haranguing you about this matter if you seek help. They will also not stop haranguing the rest of the world about this -claiming that anyone who believes otherwise is hurtful and hateful and judgmental, and kills people with their words if they mention an opposing opinion (I got such wonderful messages in my hate mail regularly).
I, on the other hand, stand here in my own tiny little corner of the internet, debating this issue. This tiny little corner is for people who care about this issue. I do not stand outside an AA meeting projecting my words through a window onto the wall behind the speaker. This site, and this page particularly are for people who care about this issue, and the effect that our beliefs about it will have upon our actions.
So even a “latitudinarian” comment that pretends as if this page stands as an assault on those who are humbly trying to change their lives (by saying essentially ‘who cares, just back off of people and let them be’) is an outright insult to me and anyone who is seriously trying to get this issue figured out.
Ok, fair enough, BUT as a human being, my response to such a marginalization of another person’s existence (whether by disease or nondisease side) is an affront to good manners and finding a more common ground, so I wrote. I can see that this forum is not for common ground, as you are here for people who care about this as an important issue. I get it, this is your corner. I would suggest that you try being more magnanimous, but perhaps there’s been too much vitriol here to be reasonable….
Best of luck
I was already irritated by the article itself; you claim to be a “cured” addict (or nobody’s REALLY an addict, it’s hard to tell what you think about it), but honestly you really don’t come across as someone who has been in the trenches and really gets the depths adiction can bring you to. You authored a well written, albeit a very biased and one sided article, where you cherry picked the few studies that fit your personal opinion. This subject is controversial and the brain is not close to being filly understood, yet you and the few PhDs you cite act as if it’s all been figured out. Then you go on to respond to this lady in an angry, bitter way, picking apart her comment and disingenuously acting like you don’t get what she meant. Clearly she was saying she doesn’t judge people’s route to recovery; she’s just happy when they get there. Maybe you just chose to quit and the rest is history. I hate to break it to you, but most addicts don’t get it so easily. In fact, you claimed that most addicts quit, and I challenge you to prove that assertion. I was a heroin addict for well over a decade, and I have known a TON of addicts. I KNOW most addicts struggle with their addiction their entire lives, and I can assure you I wouldn’t have chosen movie tickets over a bag of smack.
How many times do I have to prove it? There’s tons of data that proves most “addicts” quit, here’s a good summary of some of it: Addiction and Choice: Theory and New Data by Gene Heyman, 2013
All of the “who cares” comments are an insult. Sorry you can’t see that, but it’s clear: “who cares” means “it doesn’t matter” it’s irrelevant.” But it’s not irrelevant, and anyone who TRULY thinks it is irrelevant would have never clicked the link to come to this page. The problem is that they know the disease model is flawed and doesn’t stand up to scrutiny, but they think it’s “compassionate” or some such thing, and so it serves a purpose. So they cop out on making a call about whether it seems correct and say instead “who cares”, because they think they’d be a mean person if they agreed that it’s not a disease – and they wanna be nice. Spreading the false disease model of addiction might be “nice” or “compassionate” (in motive only) when done by someone who’s ignorant of the truth, or someone who’s mis-reasoned and made an honest intellectual mistake – they mean well. Spreading falsehoods is never nice, compassionate, or helpful in reality though- it brings destruction to those who believe the falsehoods. But when people have glimpsed the truth, and choose to ignore it – then continue to spread these falsehoods or even look the other way, I consider that recklessly negligent or even evil.
Your argument against my position is that we don’t know everything about the brain yet. of course we don’t. And in every field of inquiry there is data that has yet to be known. SO WHAT? Much is known, and none of it validates the disease model of addiction. Please, respond by pasting links to all of the articles where you use that logic against those pushing the disease model of addiction. If I see that, my head might explode.
(my previous comment is now gone, so I will send this again)
1. Re: your cited link
Heyman’s “most addicts quit” idea, from reading your cited link, seems to rely very heavily on the Vietnam veterans study. That is way too specific of an instance to be broad enough for our purposes here. And Heyman also cites Klingemann, who says that some people cannot seem to effect self-change…
“With the mushrooming development of evidence for self-change,it is easy to forget that there are many people who do not succeed at self-change. Such individuals are a forgotten but important population and warrant investigation in their own right.” (Klingemann, Continuities and changes in self‐change research, ADDICTION 105(9):1510 – 1518 · AUGUST 2010).
But this does not prove addiction is or is not a disease.
2: I did have a question…. how can we rule out that addicts are not suffering from a delusion, about the effects of their actions, their level of choice, etc.?
Definition of delusion… “Delusions are false beliefs based on incorrect inference about external reality that persist despite the evidence to the contrary and these beliefs are not ordinarily accepted by other members of the person’s culture or subculture……Unfortunately, patients with delusional disorder do not have good insight into their pathological experiences. Interestingly, despite significant delusions, many other psychosocial abilities remain intact, as if the delusions are circumscribed. Indeed, this is one of the key differences between delusional disorder and other primary psychotic disorders. However, the individual may rarely seek psychiatric help, remain isolated, and often present to internists, surgeons, dermatologists, policemen, and lawyers rather than psychiatrists.” (http://emedicine.medscape.com/article/292991-overview)
“Hyperdopaminergic states have been implicated in the development of delusions. Recently, Morimoto et al[15] reported that 13 patients with delusional disorder were reported to have increased levels of plasma homovanillic acid (HVA) (a dopamine metabolite) compared with control subjects. Patients responded well to treatment with low-dose haloperidol (average 2.7 mg/d) and showed decreased posttreatment plasma level of HVA, which correlated with the improvement of their symptoms.”(http://emedicine.medscape.com/article/292991-overview#a4)
So, would you argue that delusions are not from a diseased neural system of some sort? They are not choosing to have a delusion. And addiction may be perpetuated by a delusion (about consequences and one’s own control over future use or that one cannot survive without their substance or compensatory addict behavior) common to a certain population of addicts… like other commonly reported delusions like having been poisoned, etc. Dopamine may indeed yet be implied in a very specific belief in the idea around one’s inability to quit without dying, etc.
This doesn’t prove anything, I know, but it reminds me of the complexity of the addiction brain issue. The belief in inability to quit could be a delusion, and other factors could contribute to the substance of the delusion being weakened over time, at which time the person quits using. Maybe the hyperdopaminergic state subsides due to age or overuse of chemicals or due to other bonding chemicals when someone really bonds to the importance of family or of career. Does that mean they were not delusionally addicted during all those attempts at treatment forced by their families and during those relapses? In fact, does one’s situation at quitting time have anything to do with whether they felt they were addicted at an earlier time? One’s subjective feeling can be because of a disease or because of some other type of condition.
It seems worthy of exploration. I am sure you aren’t about to argue that mental conditions are not ever diseases.
Just know that if you comment from a different ip address/email combination, it will hold that comment until I get around to approving it. This is an anti-spam measure.
I agree with you. I 100% know that our beliefs do influence our actions. If you think you can’t overcoming something, you won’t. If you are told you can’t overcome something, and if that is all you are told, what do you think will follow? By some people – addicts – they would probably say that I was an addict in early 2000. I had a drink (alcoholic) probably 3 or 4 times per day. I had it in my coffee and I’d mix that up four times a day. After 6 weeks of that, I just stopped – on my own. My own thinking was this “What are you doing to yourself? Why are you doing this? Who is in control right now? Do you want to continue to drink like this every day, four times a day? Do you want to continue to wake up around 8 or 9am and continue to go to bed around 2am? Do you want to live like this?” I never went to any AA meetings. I was drinking my life away and after 6 weeks of being depressed I just had to stop. I had no money coming in in march 2003- but I had lots of alcohol in the house since I had bought some before I got unemployed that march. I had to wait several months before getting any unemployment benefits. I had no car, no money and alcohol in our cupboard. I drink. Then I woke up. No one told me “You are an addict, you can’t help yourself. You must go to AA meetings and rely on God.” No one told me that. No one. I believed in myself to stop. I knew I had to help myself. I knew that If I didn’t, no one else would make me stop. And since I believed that I could stop (not under any weird force – something forcing me to drink) I stopped. I believed that I had the power. And I was a Christian at the time. Imagine that. God didn’t tell me to stop. I did.
It is ridiculous that you would even consider comparing drug addiction to being a good taxi driver. How about you get a psychology degree, from a well credited institution, before you spew nonsense on the easily swayed and vulnerable public. I’m sure you do not have one, because if you did, you probably wouldn’t be insulting many of us who suffer from addiction with your false article. My first statement leads me to believe you must have some sort of preconceived notion and idea about addiction, otherwise you wouldn’t stoop as low to as making such a laughable comparison. I pity you. You must be so narrow minded as to have your own anger and insecurities to fuel this poorly written article. Until you firsthand face addiction on your own, please, spare yourself from appearing to be a judgmental fool. By the way, congrats on earning a living through a negative means by putting others down, not to mention writing articles for this funny website. LOL. Bet you make lots of money.
Funny to see a bunch of addicts getting all bent out of shape because drug use is a choice. Keep telling yourself that its a disease and see where it gets you. Wah, wah, wah I can’t help myself, I have a disease. Wake up and stop having pity for yourself. I know drug addicts, I’ve grown up around them my whole life, most are just lonely, weak-willed individuals. I could give two fucks if you are offended by my comment.
It is shocking how much a challenge to the disease model upsets people. Personally, back when I had a problem, I was happy and relieved to finally be told that I was in control and did not in fact have a disease.
I am nitpicky about mentions of being weak-willed though. I think that when people are behaving in the way that we call “addiction”, they are very strong willed. They are doing whatever it takes to carry out their will to get drunk/high. Strength/weakness is not the issue. The issue is the “addict’s” assessment that heavy substance use is their best available option in life. If they change that perception, then they will want or “will” something else, and then exercise the power to fulfill that want, moving them away from heavy substance use.
By the way Steven, I completely agree with your last statement. Also, I like the new look you’ve added to the site:-)
I wish it was, in fact, shocking, Steven that disease model sheep react so babyishly to proponents of choice over disease. We see this all the time with religious zealots who base their existence upon the thought that someone or something else caused them to be ill, and that toeing the line of whatever ideology that offers them freedom from guilt is the only option. Reason, science, proof or questioning become unacceptable, and they lead lives of quiet desperation.
I’ve been following this dialogue for about 3 or 4 years, commenting often, and have even engaged in debate. My comments have often been emotionally charged, however often they were based on my personal experience with addiction, and then recovery. I’m not a scientist, but I am an informed and open-minded individual. The reason for my comment today is that recently, I came across an article by Marc Lewis, a psychologist and former addict, and the author of a new book called “The Biology of Desire: Why Addiction is Not a Disease”. Over a year ago, and after over 5 years of participating in 12 Step Groups, doing some research on my own, and being open-minded, I came to believe that addiction is not a disease. As we know, there is no physiological manifestation of disease, or disease process that causes addiction. Lewis mentions the plasticity of the brain, or “pathways” that are formed in the brain with repeated actions, such as drug and/or alcohol abuse. I get it that these are learned patterns, and the first, and maybe two or three subsequent times a person uses, is a choice. These pathways of “pleasure” then produce a false feeling of what is good and what is needed, or perceived to be needed, substance, or in some cases, behaviors, to relieve pain, memories, and feelings of isolation and threat. I am aware that after an addict stops using that after time, these pathways can be re-forged with new and more healthy choices to relieve the same pain and emotions that drugs or alcohol used to do.
Lewis does give some credibility to the 12 Step Program’s teachings and suggestions, specifically to Step One: admitting one’s helplessness over addiction, and that when one uses, they are powerless over the substance. One has to accept that abusing substances is no longer a viable way to seek pleasure. I personally think that is the first step for anyone seeking freedom from addiction, whether it be by 12 Step Programs, or any other form of recovery. The fault that Lewis finds with the concept that once an addict, always an addict, is that hard core 12 Steppers, and the promoters of the disease theory, fail to take into account the plasticity of the human brain, which I mentioned before.
I found this article on Facebook, in a closed group for recovering Gay men in Sobriety. Someone shared a link from Ted Talks, quite enlightening and informative. Ted talks about the ways other people try and “make” an addict quit. There is an overwhelming behavior of shame, guilt, belittling, negative reinforcement thrust upon the addict. It’s a 20 something minute video, based on Ted’s personal experience with people he either knows, or loves. He made a profound mention that these actions of trying to shame an addict into stopping does not work. Based on my personal experience, I would have to agree with him. Ted also mentions, as well as Lewis, that for an addict in their active addiction, having the knowledge of whether it’s a choice to use or not, is not present. It’s not so much of it being a choice, it’s a matter of knowing if you have a choice or not. The addict, isn’t able to comprehend choice, those pathways, albeit formed by their continued use, inhibit any rational thought process. This does not mean that someone, somewhere, doesn’t see that actions of their behavior, and decide to do something about it. Some do, and find their way to recovery. Some don’t, but this doesn’t make them any less of a person, and in no way means that what works for one, should work for everyone. Whatever way a person finds relief from compulsive use of substances doesn’t matter. Yes, compulsive behavior IS a part of addiction…….firmly believing in one’s mind that they need a substance to change how they feel, and they will do anything to get that next high. The compulsion to not use has to be re-written, so to speak, by changing learned patterns and behavior, which comes only after stopping the use of substances. The compulsion component of addiction is real, and not to be discounted in any way. Why and how someone takes that first step to change their lives varies among everyone, from catastrophic consequences, jail, hospitalization and/or institutionalization, being fired from a job, or even waking up one day and deciding that this cannot continue anymore. Do not make the mistake that that it is a simple choice to stop using, it is a thought process that can lead one to make a cognitive thought process, to make changes. If anyone addict can wake up one day and decide not to use, and doesn’t do so ever again, then my hat is off to them. That moment of clarity is a step in the process for many, and the choice to stop is another “learned pathway”.
If I were an addict seeking relief from addiction, or seeking answers on how to change their lives, I would not recommend this site. I talked about shaming or laying guilt on an active user, or someone who knows they need to change, but doesn’t know how. The reason I wouldn’t suggest this site is because there is a reasonable amount of shame expressed, not so much by Steven, the author of this site, but by the many people who comment. Most disqualify and discredit those who didn’t need any kind of help to get sober. I’ve seen name calling, discounting experiences, shame for an addict’s behavior being forced upon someone who is different than they are. One’s experience is just that: it belongs to one person, and while many are similar, another person cannot discount or discredit another’s experience. That shame, name calling, belittling, acting as if they are above another just because they think they are and they could do it one way or another, and the other could not, certainly is not a way to make most anyone want to get sober. That very shaming turn the help seeking addict into more shame, and do what they only know to do to make them feel better: Use.
This site has done a lot of good for many, I am sure. It incited me to look for another view on the subject, and even more personally, it has only enhanced my recovery. If a person needs to think they have a disease to get sober, so what? How does that affect you personally? Unless you’re the kind of person who always has to be right, despite any disqualifying evidence against your beliefs or opinions, than I get it. Nothing anyone says or does is going to change your mind. This site has opened my mind, something that should be happening to the many closed-minded opinions of some of the commentators in here.
The main topic of this site has gotten somewhat diluted. Many facts or statements stated here, including mine, have taken it to a personal level, not factual. That very personal level may, and in some cases, possibly has, been the deciding factor in how an addict perceives his or her addiction. Stranger things have happened, right?
drug addiction is a disease. and im not a addict. But you will never understand what some are going through. You have never placed yourself in their shoes who how they got where they are. YES addicts had the CHOICE to do it but once it alters your mind in the reward circuit. Here put it this way; Drugs are chemicals. When someone puts these chemicals into their body, either by smoking, injecting, inhaling, or eating them, they tap into the brain’s communication system and tamper with the way nerve cells normally send, receive, and process information. Different drugs—because of their chemical structures—work differently. We know there are at least two ways drugs work in the brain:
Imitating the brain’s natural chemical messengers
Overstimulating the “reward circuit” of the brain
Some drugs, like marijuana and heroin, have chemical structures that mimic that of a neurotransmitter that naturally occurs in our bodies. In fact, these drugs can “fool” our receptors, lock onto them, and activate the nerve cells. However, they don’t work the same way as a natural neurotransmitter, and the neurons wind up sending abnormal messages through the brain, which can cause problems both for our brains as well as our bodies.
Other drugs, such as cocaine and methamphetamine, cause nerve cells to release too much dopamine, which is a natural neurotransmitter, or prevent the normal recycling of dopamine. This leads to exaggerated messages in the brain, causing problems with communication channels. It’s like the difference between someone whispering in your ear versus someone shouting in a microphone.
my point is it creates the “disease” and you can NEVER cure it it will ALWAYS be there. but you can “treat it”
I’m glad I found this. After not drinking for over 14 years and staying off crack for 2 years, I think I’m ready to make the choice today to start drinking in a normal way and using crack for fun. I’ve had my depression and anxiety under control for a while too and since that really didn’t have any affect on my drinking, and using drugs, according to what I’ve read here, I shouldn’t have to worry about whether normal use will affect those issues. I’m so glad I know I have the choice to use and that I will be able to control how much I drink and use by making a choice to do it without it causing any problems. Thanks.
Oh K-hopeful, that’s what you get from the article, that is it’s your choice, to return to a behavior you had judged against your interest previously? Suddenly that behavior becomes acceptable to you because it is no longer a ‘disease’?
Oh, I get it, you are making an attempt to argue the points made by being clever. You failed.
Choice, it isn’t just about what’s for breakfast anymore.
No I’m not “trying to be clever” unlike your juvenile statement “choice-it’s not what’s for breakfast anymore”. In the past I’ve found that when I try to drink moderately I dont. I usually seem to drink way too much. And when I plan to spend $40 on Crack I end up spending $400. So it seems to me I lose my ability to make a choice once I start drinking/using. The Clean Slate says anyone can and do make a choice to use moderatly. I need the mid-set to do it instead of BELIEVING I cant. Why are you hating on me for wanting to.
I am with K-hopeful here.
First, let’s be scientific. Studies show there is heritage with addiction. Which gene that is and how its mutated is not certain.
I am a believer that I once had an obsession of the mind and I also still have an allergy of the body. Today I understand I have a choice because I have been relieved of the obsession. I also have a choice. I can choose to not drink or get completely fucking soaked, perhaps jailed, certainly a hospital or doctor will be involved if not a mortician. There is no in between for this person. I guess I was not schooled properly.
what I forgot in the first sentence…..is this not the same for cancer or diabetes, both of which are diseases.
dis·ease
dəˈzēz/
noun
a disorder of structure or function in a human, animal, or plant, especially one that produces specific signs or symptoms or that affects a specific location and is not simply a direct result of physical injury.
Do what works for YOU. I’ve got 30 years via 12 step. Anyone who says it is a farce can eat my shorts. Use the protocol that you find works (and keeps working) for YOU!
ADDICTION IS NOT A CHOICE!!!!!!!!!!!!!! Come on! Yes, using is a choice, but NO ONE WHO HAS EVER USED SAID, “I Want to be an addict!”
SO many people use… and it was their CHOICE to use! But they are not addicts, so they can stop anytime and never get out of hand. Someone with SUD
(Substance Abuse Disorder) cannot just STOP… his/her body craves it, like you and I crave water and oxygen.
Yes, like all other diseases, with medical help or constant and continued work… the addict can be in remission.. forever. and the ” work” is a choice.. but only
once they’ve gotten to the “remission” stage. Just like picking the drug or alcohol back up “after” remission is a CHOICE! But ADDICTION is not.
My mother-in-law died from lung cancer. Smoking was her CHOICE! However… SHE DID NOT ‘CHOOSE’ TO GET CANCER! Do you get it? Her
sisters, her husband, her parents ALL SMOKED ALL THEIR LIVES…. but NOT A SINGLE ONE of them got cancer… just her. So you are telling me that my mother-in -law
chose cancer, but her family did not… THEY were spared???. My friend died two years ago at the age of 49 of a heart attack. He smoked occasionally and drank occasionally and ate Burgers and fries and Hot Dogs on the grill (charred) AND cake and ice cream (sugar). But he was NOT an addict and he was a lively HAPPY man. then BANG! Died n his sleep.
YES, he CHOOSE to eat at McDonald’s (like many people) he chose to smoke (link many people) HE DID NOT CHOOSE TO HAVE HEART DISEASE!
Millions and millions of people live like he did… and many much worse! He was a very active person.. not sedentary and a couch potato by any stretch of the imagination. Many of the choices he made “could have’ lead to his untimely death… and his hear disease… but THE DISEASE itself he did not “choose”. My mother-in-law’s lifestyle definitely lead to her death of lung cancer. BUT LUNG CANCER she DID NOT CHOOSE! I promise you.
I don’t understand why, when I give accurate examples of being out of control caused by your brain ( as in taking a breath when you know you can’t breathe in thick smoke or water ), and physical changes caused by alcohol consumption ( slurred speech, double vision, stumbling, the affect on breathing and heart rate), but the information on this site states there are no brain changes affecting our choices when we use, and if I choose moderation I can have moderation, yet you also say my APPETITE must BE moderate to choose moderation…. if my APPETITE is heavy, I will use heavy. OK do I have control over my appetite or don’t I ? Why is it Steven Slate that you don’t address these questions?
First off, there isn’t anyone screaming anything from any rooftops! I understand the frustration from many who think that since addiction has been classified as a disease, that some addicts or alcoholics use that as an excuse for their past, and in some cases, current behavior. And even more poignant, the money that goes to treat these individuals, and last time I checked, that money, or lack of it, hasn’t caused anyone harm, at least for me. Sure, maybe the money spent on that could be better spent, but the effort and money spent to debunk the disease theory is, quite simply, a waste. Also all of the effort, angst, anger and misguided opinions have to count for something. Who in their right minds wants to be preoccupied with this issue? Why does it matter why and by what means a person’s recovery is facilitated? Whatever brings a person into recovery, whether it be medical treatment, 12 step programs, meditation….whatever…..is none of anybody’s business.
It’s obvious all of here have had different experiences with addiction, whether it be oneself, a family member or friend, or just seeing it in the media. Each person’s experience and journey belongs to them, and nobody has the right to discredit it. Nobody!!! Each person reacts to a substance differently, and yes, the parallels can be very similar, but no one is exactly the same. Someone mentioned the “fight or flight” action taken by the brain. The individual’s reaction to this action is, once again, very different from another person.
I have been in “remission” as one person stated it, from drugs and alcohol for almost 6 years. I have no inclination to ever pick up again. But if I did, that first pick up would most definitely be my choice, but after that, all bets are off! I would instantaneously go right back to where I left off, and what subsequently follows, is not a choice. When I first picked up a drug or had a drink, that was a choice. I didn’t choose to be addicted, it happened without any conscious choice or doing on my part. That “flight or fight ” action…..well, in my case, as it is with most addicts I presume, the “flight” action leads to escaping, checking out, and the brain tells us that this is the only way to cope with shit. I bet some of you who adamantly prescribe to the idea that we could stop anytime we choose, have never really experienced full-blown addiction. And until you do or have, keep your rude and condescending comments to yourselves.
One more thing, I’ve always has an issue with addiction being a certified disease, and I don’t subscribe to that theory. But, many of the components of addiction that are described by the author here, are questionable. Compulsion, the analogy of the taxi driver, the claim that changes in the brain don’t have any effect on long-term recovery, and the obvious brain changes that occur while one is in their addiction are all flawed. I do believe in neuroplasticity, but those “regenerating” effects don’t occur right away. So yes, the brain can recover, but an intervention of any kind is the only way that can happen. I am not a scientist, researcher or expert on addiction. I am however, someone who used drugs and alcohol for many, many years…..like 35 to be exact. I think I know something about compulsion, resorting to the “flight” action to make me feel better, and I can read and comprehend research, reports and findings. One more thing…..in the section “Why does it matter……”, that is the question. It doesn’t. It only matters to those who think they know better, and are obsessed with trying to manipulate how and why a certain percentage of people get sober. Put a little more energy into global warming, the plight of the homeless, or even electing a President who’s not psycho. There are much bigger things than trying to prove something that’s not worth proving.
I agree with you Clay that nobody has the right to discredit any method that worked for any person that was able to get them away from the misery and suffering that goes hand and hand with out of control active use/addiction. If it works for you, do it. If you want to try moderation, try it. I also have 35 years of active drug/alcohol use behind me…. What worked for me also erased the overwhelming anxiety and depression from my life. I needed to be taught how to deal with those problems and how to not give in to that compulsion to use. Thankfully I wasn’t just told….”choose not to”……. cause I did that a million times over and over again in that 35 years without success and now I have knowledge about how my brain and body works. Saying things like “It won’t make a bit of difference if you walk away from your 12 step program or not.” Really? You don’t know if that’s true for everyone. Some people need AA/NA, some people need to be taught moderation. Mr. Slate I truly think one of the silliest things I’ve ever heard is alcohol and drugs don’t affect our brain in some way. If they’re affecting our central nervous system they’re affecting our brain. To say we all have a choice BUT that choice is affected by your appetite and whether it’s moderate or heavy — that’s just talking out of both sides of your mouth – it’s a complete contradiction that you have yet to explain why it’s not. And CBT & CBE are two entirely different things? No they’re not. Cognitive Behavior Therapy is taught by therapists, Cognitive Behavior Education is taught by non-certified therapist. The concept of each is the same. Funny how that method is used by those whose believe in the disease concept and by those who don’t in an effort to help those who need help dealing with addiction.
1) Wanna give me a quote on where I said that “alcohol and drugs don’t affect our brain in some way”???
You can’t give me a quote because I said no such thing. Read carefully please, or else you might look as if you’re intentionally distorting my views.
2) You said that “To say we all have a choice BUT that choice is affected by your appetite and whether it’s moderate or heavy — that’s just talking out of both sides of your mouth – it’s a complete contradiction that you have yet to explain why it’s not.” Yet anyone who honestly reads what I’ve written on the subject would realize there is no contradiction there Substance “Appetite” as I have presented it in my article on moderation is a function of your view of the benefits of the substance:
I did not go into depth on how to change the beliefs that fuel a large appetite, because frankly, that could be a book full of information challenging each of those beliefs. You change your beliefs by challenging them. You change your preferences by finding things you can prefer better. I provide some basic challenges in another article I linked to within that article.
You choose what you believe, thus, developing a moderate appetite is a matter of choice. Again, as I wrote in that article you’re referring to:
I can’t hold your mind by the hand and do it for you. You can only really do this for yourself. Are you ready to believe the effects of drugs and alcohol are meaningless cheap thrills that pale in comparison to what else you can create in your life? Or will you go to a meeting tonight and reinforce your belief in their magical powers by talking about how they were the only thing that could ever make you comfortable in your own skin?
The choice is yours.
-Steven Slate
I apologize…. What I meant to say was you tell us that drugs and alcohol use never change our brain to take away our choice…. Our brain is in control of the choice we make…. that never changes. In Successful Moderate Drinking/ Substance use – Who can Moderate, When, and How? You say… “people choose to take every drink or hit of a drug or alcohol that ever enters their bodies. Seriously….. They choose the first drink, second drink, third, fourth, fifth, sixth, seventh, eighth, ninth, tenth, eleventh, twelfth, thirteenth, fourteenth drinks, and so on” and there is “the myth of loss of control” So this is true even in a blackout? One can’t control the blurred vision, the slurred speech, the stumbling, but through all that you can control if you take another drink. Bartenders and waitstaff are taught to recognize a patron who has had too much and cut them off precisely because that person is beyond their capacity to know and choose it’s time to stop, people drive drunk and kill their own friends and relatives because their brain ISN’T ABLE TO TELL THEM NOT TO GET BEHIND THE WHEEL. How you walk, talk, see, and the ability to make a safe decision is GONE but your choice is not?…….THAT is the silliest thing I’ve ever heard. Whether I’m at a meeting or reading your blog, at least I have the ability to recognize when something is complete bullshit. And everything I’ve heard from others in recovery and/or treatment is we DON’T need drugs to feel comfortable in our own skin!
Hi K – You’re talking about two different kinds of capacities here – physical versus mental. We have much evidence of alcohol’s effects on our physical abilities, but it’s effect on our mental abilities is not so clear. Think of it this way – alcohol may affect your ability to judge whether you’re speaking loudly or softly enough in a given situation, because it has impeded the operation of your sense of hearing perhaps, and so your sensory judgment (am I speaking loudly or softly) is impaired. But this is not the same thing as your “moral” (I know it’s a hot-button term, but it’s the most appropriate word I know of here) judgment being impaired – that is, your judgement of a given choice being a good or bad one. E.g., “should I tell an off color joke right now amongst these people? – that’s a far different question than “am I speaking too loudly?” – these are categorically different types of judgments.
What we know about moral judgments while under the influence of alcohol is that in cultures where drunkenness is believed to lead to aggressive, violent, inappropriate, or overly sexual behavior – then people often behave that way when drinking. That is to say, people behave as if their moral judgment is impaired. But in cultures that don’t hold these beliefs, people do not become aggressive, violent, inappropriate, or overly sexual when drinking. That is, they do not behave as if their moral judgment is impaired. If alcohol truly impaired moral judgment, then people should show impaired moral judgment whether or not their culture believes that alcohol does so. This is clearly not the case, as demonstrated in the wonderful book I recommend everyone to read: Drunken Comportment, by Macandrew and Edgerton, 1969. They gathered ethnographies of drinking from all over the world to demonstrate this point.
Take away point is that we shouldn’t conflate sensory judgment with moral judgment. And remember, this isn’t a denial of the fact that many people do in fact behave differently when drinking, but it’s a different take on the cause. I’m suggesting the cause is belief based rather than pharmacological.
As for blackouts, they are somewhat of a mystery, but we know that the brain stops recording memory during a blackout. But just because you don’t remember making a choice doesn’t mean you didn’t make a choice. Kind of like driving your car home from work the same way every day. As long as the trip is uneventful, your brain stops committing it to memory after you’ve done it several times. But when you get home, and don’t really remember choosing to accelerate your car, press the breaks at a stop light, or change lanes to pass a slower driver doesn’t mean that you weren’t in control of yourself and that you didn’t choose to do all those things. You did choose them although you don’t remember the details of doing so.
Best,
Steven Slate
Steve,
I have been off and on to your site for many years now. Your comparisons are mind boggling. Now we are comparing blackouts to driving home. HAHAHAHAHAHAHA. It is hilarious! Where has my boy, Kevin, been? I always love reading what he has to say.
Cheers Mate,
Matt
Matt – are you capable of conceptual thinking? I’m using analogy here to demonstrate principle. Get over being incredulous, and think about what I’m saying. I laid it out there. During blackout, the brain stops recording long term memory. During oft-repeated activities, the brain ceases to record long term memory as well. Hence the driving example. Are you not in control of yourself while driving home from work even though you don’t remember it after the fact? I believe you are in control in that situation. If I am correct, then loss-of-control isn’t a universal part of experiences where long term memory wasn’t recorded (such as……. A BLACKOUT!). I’m not saying this is the end all be all of discussions and arguments about blackouts, but I believe it is a valid challenge to the assumption (YES – ASSUMPTION) that because you don’t remember what you did when you got drunk last night then you must not have been in control of what you did.
Are you gonna think about this, or just continue to be incredulous?
-Steven
HAHAHAHAHAHAHAHA. I didn’t get drunk last night, but I took a bunch of oxys and Xanax, and I didn’t remember anything. I do remember taking my kids to school this morning, though, like I do every morning, and that was over 4 hours ago. Should I have forgotten about taking them to school by now? Is that long term? I bet if I did some more oxys and Xanax right now, I would forget that I took them to school.
Matt
No I actually wasn’t confusing “sensory abilities/physical changes and moral judgement”. I think I made it pretty clear my point was if we can’t be in control of our physical selves how are we in control of our choices.
” I’m suggesting the cause is belief based rather than pharmacological.” ….. Just because you SUGGEST it, doesn’t make it true.
When you talk about driving home those things you describe are called “muscle memory” and in fact it’s how are brains function when we do something over and over again, be it pitching a baseball, to dancing a tango, to driving home.
Blackouts are not “somewhat of a mystery”….In a blackout Alcohol acts as an agonist of the GABAA type receptor, leading to memory disruption. There has been an awful lot of studies and medical advances since 1969 on how alcohol works on our brain and how it affects different human beings, including gene types that put you at higher risk of developing brain damage from alcohol consumption.
Sorry but there is medical evidence all over the place that anyone can look up starting with US Department on Health and Human Services and National Institute of Health on alcohol brain diseases.
You can’t just have brain changes that affect our physical abilities and not have an affect on the rest of our being, what we do, and how we act under the influence…… no more than one can choose to not take a breath while underwater there are things that we cannot choose, and things that affect our brains and our abilities to choose.
Steven if you were a lawyer you would make an argument that if a woman was raped while in a coma, that doesn’t mean she didn’t choose to have sex.
Hi K,
Yes, you are confusing the physical effects of alcohol on the physical actions of the body with the activities of the human mind. You said:
and…
And in each of those sentences you lump two categorically different abilities together. Walking, talking (not the message and word choice part of it, but the actual speech part of it), and seeing are all these sort of mechanical physical abilities. Making a choice however, is a very different thing. We make choices by weighing potential options and judging what’s best for us. We juggle information, project outcomes, et cetera.
You haven’t established that “the ability to make a safe decision is GONE.” You only justified it by referring to a law about bartenders being held responsible for serving the drunk – you didn’t actually refer to any logical mechanism by which the ability to make a safe decision could disappear, nor did you offer any scientific data to demonstrate it.
It is not quite the same thing to say that alcohol has slowed down our nervous system in a way that we’ve lost our balance and now will stumble when we try to walk – than it is to say that alcohol all of a sudden implanted the idea in your head that you should walk to the bar to have another drink, cheat on your significant other, or pick a fight with someone. These are all active choices, and it’s not as if we would just being doing these things all the time except that we are able to stop ourselves from doing so – and that when we drink, our ability to stop ourselves is impaired just as our ability to receive signals from our eyes is impaired.
I get it though. You think that brain=mind and thus alcohol affects brain thus it affects mind (or maybe you’re a materialist who doesn’t believe in mind – idk). But again, Drunken Comportment amassed reams of data demonstrating that what we think of as impaired decision making by drinkers doesn’t happen where it isn’t believed in, or that it happens right within the bounds of what a given culture is willing to tolerate. Yes, that book was written in 1969, but no one has compiled any data that discredits its thesis. Again, it’s thesis seems to be that the pharmacological action of alcohol isn’t causing these “bad choices” but that people are carefully choosing within what is acceptable within their cultures beliefs about drunken behavior.
Decision-making (i.e. choice), is categorically a different thing than seeing, speaking, or walking. If you have reliable information that verifies that alcohol impairs decision making (and that it deals with the problem of culture brought up by Drunken Comportment), I sincerely implore you to post links of it here, as I am highly interested in this topic and have been trying to learn as much about it as possible. Appeals to authority won’t do, and mere theory will be judged as best as it can be judged without the necessary data.
I will address some of your other points in another response.
-Steven
Hi K,
You quote me, and mock:
Yet I have offered up an actual source and reference to data, and explained that data and how it adds up. You have only asserted that the ability to make a decision is lost, and have vaguely referred to HHS and NIH without directly explaining what data they have that is relevant to this or how the ability to make safe decisions/choices is lost.
“It is not quite the same thing to say that alcohol has slowed down our nervous system in a way that we’ve lost our balance and now will stumble when we try to walk – than it is to say that alcohol all of a sudden implanted the idea in your head that you should walk to the bar to have another drink, cheat on your significant other, or pick a fight with someone. These are all active choices, and it’s not as if we would just being doing these things all the time except that we are able to stop ourselves from doing so – and that when we drink, our ability to stop ourselves is impaired just as our ability to receive signals from our eyes is impaired.”
You say “our ability to stop ourselves is impaired” and that means our ability to make a CHOICE is impaired. (I never said alcohol implants choices in your head.)
Oh and I used your technique of googling and googled “Alcohol and Brain disease” ….. there’s a lot of information that refers to COGNITIVE FUNCTION and how it’s affected by alcohol, By definition Cognitive functions encompass reasoning, memory, attention, and language.
REASONING…. how we make choices, why we make choices. The action of thinking about something in a logical, sensible way. Also “Alcohol Related Brain Impairment” and how it affects our ability TO THINK. So even though I have decreased cognitive function and have affected my ability to think…. I still have the ability to make a choice?
I’m not mocking you…. I’m trying to make a valid point and you use “spin” to tell me I’m wrong and in the same reply you even say “OUR ABILITIES ARE IMPAIRED”
Hi again K,
That you said this, really shows how much you don’t understand what I’m saying at all:
And indeed, that you think this translates at all shows how confused you are about what is going on with heavy substance use. Who is the rapist in the drug and alcohol use while blacked out situation? Is someone forcibly putting those drinks and drugs into your body? Of course not. The individual who is blacked out (i.e., not recording memory due to the alcohol’s effect on the brain – or some other sedative’s effect on the brain) is clearly drinking/smoking/snorting/shooting the substances into their own body.
And this is where the disease model has such ridiculous gaps. We always talk about “losing control”, but losing control to what??? If you’re not in control of yourself, then who or what is? Are you possessed by a demon? Are you possessed by alcohol? Does alcohol have a will of it’s own…… e.g. “the drink takes a drink”??? That’s absurdity.
I’m getting a lot of useless rhetoric out of you. And you’ve clearly designed it to get an emotional reaction out of people – after all, now I’m a victim blamer just like those rape victim blamers, right??? But you’ve offered up no perpetrator.
Can you make a sound argument, or just rhetoric?
-Steven
Hi again K –
I don’t appreciate this:
Because you tried to make me look as if I’m ignorant about blackouts – but then YOU OFFERED UP THE SAME EXACT FACT ABOUT BLACKOUTS THAT I STATED ALREADY. You just dressed it up in scientific language. As I stated, in my FULL QUOTE:
You literally said the same thing as me, with the addition of jargon, and the addition of no other points about what really happens during a blackout other than “memory disruption”, and thenpretended that I’m a dummy. You are scum. I am sorry, that is just a complete and total scum, bad faith debate tactic. I have no respect for that crap. And for the record, unless you can explain people’s subjective experience of a blackout, which you can’t, because you can’t get into their mind at the time to experience, and they can’t remember it to tell you what they experienced, then YOU MUST AGREE WITH ME THAT BLACKOUTS ARE SOMEWHAT OF A MYSTERY.
Bye Hater,
Steven Slate
HaHa you’re the only hater…. I got that quote about blackouts directly for the NIH website… they know the actual brain function that’s happening when one has a blackout…. I can’t help it if you don’t like someone who actually has looked thing up to prove you can’t make choices under the influence. And “because you can’t get into their mind at the time to experience, and they can’t remember it to tell you what they experienced” how DO YOU KNOW THEY’RE ABLE TO MAKE CHOICES?????
Wow, really? You resort to name calling like that and you’re a professional? Talk about disrespectful! That’s juvenile behavior used by children and it reflects on your credibility…. not mine. Anybody who can find your website can easily find the information I used to make my point. And I did it WITHOUT personally attacking YOU.
the changes in the brain which they show us are not abnormal at all
people change their behavior IN SPITE OF the fact that their brain has changed in response to repeated substance use
there is no evidence that the behavior of addicts is compulsive (compulsive meaning involuntary) (point two addresses this, as well as some other research that will be presented)
Steven,
Isn’t it possible that substance abuse falls in between the two opposing views of a 100% free will choice and a compulsive involuntary behavior?
That the brain sections responsible for pleasure/reward and/or making good choices are compromised by substance abuse, but not disabled.
People with substances have neither what we would call “normal” free will, but neither are they compulsed to use. Their brain function has been comprimised to the point that rational decision making is more difficult but not impossible.
As to points above:
* changes in brain are not abnormal. Have to define abnormal. If you’re tyring to say this is an image of a normal brain compared to a non user, I’d say wrong. If you say the brain adapts to various inputs, and this is a “normal” brain adaption to meth, possibly correct. If we assume the brain reacts and adapts to all inputs, couldn’t we also say that some of these adaptations tend to be positive, some benign, and some negative. All within normal brain reactions, but we could place albeit subjective judgement as to whether the adaptions are useful/positive, neutral or negative based on the behaviors.
*people change their behavior in spite of substance abuse. True, which shows that brain changes do not produce involuntary/compulsive action that is 100% outside of the control of the user. But it doesn’t prove the point that free will/choice hasn’t been diminished in some way, that the substance abuse hasn’t caused any damage to what we consider normal brain functioning affecting decision making. I think making poor choices despite repeated and severe negative consequences tend to suggest something is going on that has diminished but not completely controlled normal decision making.
* no evidence that actions are compulsive involuntary. True but again, that’s an extreme threshold, to imply that brain damage results in complete loss of control and that choice, any choice, is no longer possible. I don’t know if anyone is really saying that.
Clay,
It’s “none of anybody’s business” yet here you are going on and on about it. You’re giving this issue that supposedly doesn’t matter quite a bit of thought and attention. Why? You’re just spouting rhetoric. And you really have the balls to say that nobody’s screaming it? I’m sick of these dismissive and frankly self-contradictory comments from you and others. So I addressed this one basic point in a new post: The Disease Propaganda Never Stops. Or, yes it is being screamed from the rooftops.
The rest of what you’ve written has been addressed here a million and one times, and I won’t get into it, because I’ll just be countered with more rhetoric.
Since the issue doesn’t matter to you, then I assume you won’t be commenting here anymore. Best wishes,
Steven
Steven, first off, thanks for linking my comment to your section on disease and propaganda. Finally, a link to something I wrote, on the web! Oh wait, I am published on the web. I have a website of my own, but not on this topic. I believe that I have a noteworthy and valid comment to make, but before I do that, I wanted to address your reply to my latest comment. The “it’s not anybody’s business” line from my comment dated Sept 30, by that I mean, why, by what means a person gets sober, how those means are facilitated, and the personal experience of the individual is none of anybody’s business, it is private (unless shared) and should not be discounted or dismissed. And yes, I had the balls (pretty big ones) to say that they’re not screaming from the rooftops. While there is ongoing discussion all the time, the links in your new section are one, very informative, and two, not what I would call “screaming”. Nobody (other than researchers etc.) would know that discussion is even going on unless they actually Googled it. It really doesn’t amount to screaming, may a little loud talking at best.
That was noteworthy, but here comes the more substantial point, or comment, I want to make. I came around to believing that addiction is not a disease. I am usually one that is hard to convince of something I feel passionate about, yet I did a little research, put the pieces of the puzzle together, and re-aligned my way of thinking. Thank you Steven, you were part of that process. The things I’ve disagreed on are some of your analogies (others have made comments too), and your theories presented in relation to choice and compulsion. There is book out, just published called “Lust, Men and Meth”, by David Fawcett, PhD. I started reading it recently, and not more than one chapter into it, was amazed at what is presented. I think I may not have been specific enough in some of my comments when it comes to a specific drug: Meth. As you know, it is a drug like no other, and when it comes to recovery from that drug, no recovery (or willpower) can be assimilated to any of the information and theories presented here. This book discusses and presents ideas relating specifically to choice and compulsion. It is overwhelming just how much this book makes sense to me. I guess the point of this particular comment is that when it comes to addiction and recovery, what is stated here has no relevance to meth. Meth is a drug all unto it’s own. Maybe you’ll check it out, maybe not. It’s worth a good looking over. I won’t be posting here anymore, I think I’ve made my point, whether rhetorical or not. I have my new site to look after. Thanks for all the insight Steven.
I’m a recovering addict, for myself and many others I’ve spoken with the belief that i have a disease has been very damaging. I tried to get clean for 5 years believing I was diseased and powerless. It was because of this belief that I failed and when I relapsed, I relapsed hard because I believed I had no choice but to keep compulsively using.
I’m clean now and no longer desire drugs. This is only possible for me today because I no longer believe I’m powerless or diseased. I’m not saying to stop using is a simple choice but it is a choice. If people recover believing they have a disease good for them. I wouldn’t want to take that away from them. However for myself I’m grateful money is being spent to disprove the disease model and that information like this article exsist. If I still believed addiction was a disease and I was powerless I think I could be dead right now.
You should’t be able to decide whether it is a disease or not unless you’ve gone through addiction yourself
No one “decides” whether addiction is a disease or not – it’s a matter of whether it objectively fits the definition of a disease or not.
I don’t need to cross the Connecticut River to determine whether it fits the definition of “ocean” or not. I don’t need to be able to swim. I don’t even need to visit New England. I need merely to review the established facts about the Connecticut River, and judge whether it fits the criteria of “ocean.” Clearly, it does not.
What I do find tremendously interesting in reading through this thread is the devotion to one side of the issue people stand on, when really what all this boils down to is a definition. Definitions change, Pluto used to be a planet until the definition of “Planet” changed, We see an alarming increase in rates of Autism in the United States, not because it is increasing in frequency, but because we changed the definition of “Autism”. Maybe at the core here is that the definition of “Disease” needs to be updated. To paint with an overly broad paintbrush, if you do agree with the author’s assessment of “choice” regardless of substance abuse type, by definition then, anyone who dies from substance abuse is not a victim of their “disease” (as discounted by the author), but instead have chosen to commit suicide over a long drawn out period through substance abuse (or possible very short term in the case of an overdose). When the partaker of a drug knows good and well the potential or likely lethal outcome of their substance of choice, how else can you define it other than the choice to commit suicide? Wait a moment however, when we look up the term “suicide” we regularly see it defined as a Mental Health issue (and by current definition Mental Health issues are not diseases). Again you can argue that committing suicide is a choice, but when you hear things like “the side effects of XYZ drug include increases in suicidal thoughts” verify that drugs can and do alter ones ability to make clear and rational decisions (choices) you find yourself in a very sticky middle ground that yes…by DEFINITION, issues of the mind are not diseases, but though the author’s argument of “disease” has been satisfied, it does not excluded the fact that substances can alter ones ability to make choices. The XYZ drug doesn’t allow the person to chose if they are going to have these thoughts…that is a simple matter of chemistry. You might then add…well they have the choice to commit suicide or not, regardless of how many suicidal thoughts they have…but I would posit the idea that, with enough thought, actions tend to follow suit….so in summation, what I hear is that the solution to this argument might be best alleviated by changing the definition of “disease”….if we can do it to a planet, we can do it to for addictions.
We know that substances like alcohol can damage organs such as the liver and heart. Damage to the liver or heart, for example by alcohol abuse, would probably be considered a “disease” even though the organ was damaged by decisions of the individual. Most heart disease has a lifestyle component, as does diabetes and some cancers. Yes, choices are made, to eat the wrong foods, to not get sufficient exercise, to smoke, to drink to take drugs, but if the organ is damaged by “choice” then we still consider resulting damage to the organ a “disease”
Damage to the organ called the brain is simply more complex, compared to the liver or the heart. We don’t have a great understanding of exactly how the brain functions although we are learning more all the time. We don’t understand how repeated use of substances can damage the brain, or what that damage might look like. Brain scans are beginning to give us more information.
The job of the heart is to pump blood. The job of the liver to remove toxins. The job of the brain among many functions is to make choices and to get us to repeat activities that provide reward/pleasure. And since some of the brain functions are related to decision making/choice, and pleasure and reward, damage to the brain that affects it’s functioning can be mistaken for a person simply making “bad choices” But if the part of the brain that makes choices is damaged, if the function of that part of the organ is simply to choose, then it’s not a leap of faith to assume that damage to an organ designed to help us choose would result in “wrong” choices. The function is to choose. Damage the organ designed to help us choose, and bad choices will result.
If substances do damage to the normal function of by brain, is this a “brain disease?” Well if substances do damage to your heart, I’d think you’d call it “heart disease” so in the same way, I’d say yes, if we can show that substances damage areas of the brain related to decision making /choice and to reward/pleasure, that damage could be considered a “brain disease” While the organ may continue to function at a less than optimal state, if it’s damaged it’s also not functioning normally and “bad choices” would be one normal expected outcome.
We know that substances like alcohol can damage organs such as the liver and heart. Damage to the liver or heart, for example by alcohol abuse, would probably be considered a “disease” even though the organ was damaged by decisions of the individual. Most heart disease has a lifestyle component, as does diabetes and some cancers. Yes, choices are made, to eat the wrong foods, to not get sufficient exercise, to smoke, to drink to take drugs, but if the organ is damaged by “choice” then we still consider resulting damage to the organ a “disease”
Damage to the organ called the brain is simply more complex, compared to the liver or the heart. We don’t have a great understanding of exactly how the brain functions although we are learning more all the time.
The job of the heart is to pump blood. The job of the liver to remove toxins. The job of the brain among many functions is to make choices and to get us to repeat activities that provide reward/pleasure. damage to the brain that affects it’s functioning can be mistaken for a person simply making “bad choices” But if the part of the brain that makes choices is damaged, if the function of that part of the organ is simply to choose, then it’s not a leap of faith to assume that damage to an organ designed to help us make good choices would result in “bad” choices.
If substances do damage to the normal function of by brain, is this a “brain disease?” Well if substances do damage to your heart, I’d think you’d call it “heart disease” so in the same way, I’d say yes, if we can show that substances damage areas of the brain related to decision making /choice and to reward/pleasure, that damage could be considered a “brain disease” While the organ may continue to function at a less than optimal state, if it’s damaged it’s also not functioning normally and “bad choices” would be one normal expected outcome.
Sorry, didn’t mean to duplicate post. Your site kept giving me a 404 error on each and every post.
When someone takes a substance knowing it could cause death doesn’t mean they are committing suicide or that they aren’t choosing to take the substance. All it means is that they are willing to take the risk for the perceived benefits. They might feel anxious making the choice (light I did) but they don’t really believe that they will die. Take base jumpers for example. There’s a good possibility of death but people choose to do it because they believe the odds are on their side.
If an alcoholic was sitting at a bar after already triggered the “phenomenon of craving” and someone put a gun to their head and said ” if you drink that drink in your hand I’m going to pull the trigger”. Do you think the alcoholic would take that drink? Unless he/she actually wanted to commit suicide I’m willing to bet they would find the willpower and make the choice not to drink,
Really?? Because something has been your experience you are a medical professional. So because I haven’t experienced cancer I have no right to call it a disease?
I have to admit, some of the comments I’ve left here have been motivated by anger and resentment. It wasn’t until I read a post here from Justin Thompson (which I think may have been deleted), that I realized why I get so worked up. It’s not that I disagree with every single aspect of this article. And it’s not the information presented, and whether I agree with it or not. It’s about how it’s presented. I am going to copy and paste the last paragraph from Justin’s post, and comment on that.
“Lastly, when writing such an informative article stressing one’s own opinions with such merit, I humbly offer a suggestion: Making truth statements in the form of an informative essay/ article can put oneself into a predicament of clashing opinions and contention for argument. One might consider using English Prime as a method to articulate an educated opinion without passing it off as biased fact. This way one could present an option for thought without drawing oneself into lengthy, pointless debates on the validity of one’s opinion. I, personally, agree with several points in this article. Although, there are some that I do not agree with”.
My dad always used to say to me, “it’s not what you said. It’s how you said it”. There is a lot of great information here, not all I agree with. This site did open up my mind to see a different way of thinking, and to decide for myself, that addiction is not an actual disease. The way this article is written and presented, just as Justin claims, in a way that incites debates, arguments, negativity and even the threat of being banned from the site. Presenting facts is one thing, biased facts are another. They leave no wiggle room, or an alternative other than the opinion, whether fact based or not, being stated. This article is written with the intent, in my opinion, to assert that this is gospel truth, and that addicts struggling for sobriety are less than for not subscribing to this presentation. I have read and re-read this article many times, and while there are brief glimmers of compassion and understanding for the suffering addict, it clearly has overtones of shaming and persecution. Addicts, from my personal experience and that of others, don’t need preaching or a laundry list of why they did this or they can’t do that.
I get it. Addiction is a serious problem, and research and investigation are important. So is recovery. I’m going to make a statement I’ve made before, and that is recovery, while it is facilitated with the help of countless other people, is a personal and private thing, and the means by which one recovers should not be shamed or discredited. I by no means mean to be disrespectful, I admire your intellect and passion. But intellect and passion don’t necessarily equate to understanding and compassion.
Great. Another lecture on tone. You know you’re welcome to stop visiting this page if you hate the tone so much Clay. You really are. Change the channel already.
Is that a logical fallacy or something? I didn’t like the way you said 2 + 2 = 4, so your answer is wrong. Two plus two now equals five!
If you’re going to criticize the article on tone, then at least cite some examples from the article that demonstrates its horrific tone!
But you haven’t done that. Like Justin (whose comment was not erased btw), you criticize me for (GASP!!!) believing my argument and conclusion is correct, and having the gall to present it as such. I’m sorry I’m such an awful hateful person. How dare I think that I could, should, or even dare have the right to believe in a conclusion. I should just think that there is no correct answer to anything.
Wouldn’t it be such a better world if I were just humble, and didn’t believe there were right and wrong answers to things? Then I could reach under my sink, and pull out a bottle with skull and crossbones on it, and think to myself “is anything really poison? How dare I be so arrogant as to think I know what’s poisonous” and then guzzle the chemicals I keep under my sink. Would I die? Who could say? I certainly won’t even think about taking sides on that issue anymore, because it would be so impolite, and it would invite arguments. So I guess I’ll just drink all the chemicals under my kitchen sink.
You keep saying you’re done here. And I refrained from responding to your lecture about “discrediting” people’s recovery last time. That’s a statement that paints me as some big bully but means absolutely nothing. Show me what you’re talking about when you make that claim, now that you’ve felt the need to come back here and make it a second time. Quote me, and explain how my words “discredit” or “shame” people’s recovery so that I can answer to it – or retract that accusation. I don’t appreciate such smears. I am the one who people constantly try to discredit here – people telling me that I was never a “real addict” so I don’t know what I’m talking about. YOu can see one such comment literally right above yours where some ignoramous who probably didn’t even read the article or bother to learn about the author of the article said “You should’t be able to decide whether it is a disease or not unless you’ve gone through addiction yourself.” And then there are all the accusations that my words are killing people. This and far worse in disgusting hatemail is what I deal with routinely. Yet by saying that addiction is not a disease, I am “discrediting” and “shaming” people? Or how am I doing all that nasty stuff? Is it just a smear, or can you make your case???
What I cite as discrediting or persecution may interpret something totally different to someone else. You say tomato and I say Tomah-to! You’re a pompous arrogant ass Steven. I am done. Please block me.
I’m pompous and arrogant because in my article I said what? Should I have followed up every sentence with “but I don’t know” or “I could be wrong” or “I don’t mean to hurt your feelings if you have a different opinion” – or what??? I actually do tons of defending against hurting people’s feelings that you may not even realize, but I really can’t do it all, and it isn’t my responsibility to do any of it. This article is so straightforward, and just walks point of fact through the issues. I don’t put anyone down, except perhaps Nora Volkow – and that’s debatable, because I just basically say that she’s wrong.
This article is not about feelings, it is about facts. But I have been accused of moralizing to people since I published it in 2010. I have been accused of “being judgmental” and all of that crap. I have been accused of saying a bunch of things that I never said in the article and don’t believe in life – so much so that I added a section outlining those things that I didn’t say and don’t believe – in the hopes that I would stop getting attacked for those things I didn’t say and don’t believe maybe if some people who came to this page and commented bothered to read the article. You’re one of the few who’ve taken the time to read and think about it, which is why I’m shocked to keep getting the tone lectures from you with no backup.
I think you’re oversimplifying to serve some emotional need in yourself, Mr. Slate. I want you to know that you have a choice in this. It is within your control to re-examine the phenomena you’re discussing and to present them in a more balanced and a more intellectually honest way.
Oh yeah; you can never surf the web without finding these types of articles; random, “tough”, dudes who’ve overcome their impediments, while neglecting to cater to the emotional damage done, spew callous claims at those still at the bottom.
I’m not going to bother going at “it” in as fancy a way as you did. All I’m going to say is, an addict has as much choice not to engage in the addictive behavior as an Aspergers child has not to be short tempered. Addictive behaviors are rooted in emotional issues–I bet you know this; so the addictive behavior serves as release. Cut the addiction without “cutting” the issue and you have a self-destruction–literally; like a mad dog biting itself! Not to mention not engaging in addiction required willpower, which is energy. As willpower depletes, relapse comes knocking back at the door; not to mention there are thousands other activities in each of us’ lives that require just as much willpower if not more. Is that then a wonder that a lot of people battling addiction relapse so frequently!? We relying on such a scarce resource that willpower is to serve as backbone for many aspects of our lives! And as willpower depletes, frustration builds up–which makes it so your next relapse is always very likely going to be stronger than the previous one.
I hope this gibberish will make sense to anyone who reads it.
I was taught that to be a disease a PATHOGEN must exist. To tell drug abusers they have a disease is very defeatist. People make bad choices. Many overcome these bad choices, but please don’t give them the “it’s a disease!” out.
Surely in being taught, you were taught that dictionaries provide help on questionable definitions.
As for requiring a pathogen…. here’s the definition of disease
dis·ease (di-zēz’),
1. An interruption, cessation, or disorder of a body, system, or organ structure or function.
See also: syndrome. Synonym(s): illness, morbus, sickness
2. A morbid entity ordinarily characterized by two or more of the following criteria: recognized etiologic agent(s), identifiable group of signs and symptoms, or consistent anatomic alterations.
See also: syndrome.
Pathogen:
An agent that causes disease, especially a living microorganism such as a bacterium, virus, or fungus
Before you down on people, check your definitions. Whether addiction is a disease is up in the air. It doesn’t really matter to me as long as someone can get it arrested.
Please don’t assume that 12 step programs don’t work. We are taught that we have a disease and we are not responsible for it, BUT we ARE responsible for our recovery. It is up to us to WORK the steps and LIVE the steps and the ONLY people that relapse, are the people that don’t work steps, lie in their step work, etc. It’s the addicts NOT working the program that fail, the program is flawless. 😉 Don’t try to argue poor statistics either, you can’t take statistics on anonymous people. 🙂
I just corrected the other guy for his bad definition of diseases being caused by pathogens, so now I’ll say to you, no program is flawless, not the bible and not the 12 steps or AA big book or NA basic text.
The sexism, really chauvanism, in big book alone makes me cringe. NA text is better. But these all have issues, so do anti disease programs.
Take the good, take the bad, take em both and there you have the facts of life.
Wow, I am a 56 year survivor of what was said to be terminal cancer, I didn’t choose to have cancer, cancer chose me, THAT is a disease, IT takes over your body, you don’t feed it to yourself voluntarily. That being said I also have a heroin and meth addicted son. He CHOSE to do the ILLEGAL drugs, he CHOSE to continue to use, he CHOSE to go back to doing them even after completing the rehabs (several). He didn’t just wake up one day and his brain was out of whack so he said I think I’ll try Heroin or Meth to get my brain right. He, like many others learned about drugs from friends, peers, TV, family or parents. Your brain just doesn’t crave them unless you start using them and feeding it to the brain. As I see it addicts START the process by choosing to do the drugs, then it gets out of control and then it whacks out your brain and it’s function. THAT IS WHY THEY ARE CALLED ILLEGAL DRUGS!!! It starts as a choice and ends with wacked out brain function, PERIOD. I have heard every bullshit, lame excuse in the book but it always, always, always comes back to ” he chose to start again”. Yeah I sound like a cold hearted bitch of a mom, but after years of being used, lied to, abused, stolen from, hated, and worse I get tired of hearing addicts, including my son, saying it is a disease and it’s not my fault. BULLSHIT. I have seen all things you do to yourselves thru sober eyes, trust me it is bullshit, it is your fault. It is also NOT hereditary, BOTH my parents were addicts, one alcohol and one doctor prescribed anti depressants, and it never caused me to be an addict. So, yeah, sorry but I 100% agree it is a choice and not a disease.
Oh, you seem like a copy and paste kind of person to me with no real understanding of the human brain or addiction. Have you ever been an addict? I would also like to point out the RISK FACTORS of addicts. And children who are exposed to drugs at a young age. Do some research on that. You are misinformed and naïve. I apologize if this truth is too straight forward for you. You obviously do not know much about this and you should not speak on it. Please do some extensive research and then decide if you want to post an ignorant-sounding article such as this one. Also, please stop copying and pasting other people’s opinions as your own and come up with your own bullshit.
Sincerely,
A student of Duke University in Neuroscience.
A Drug and Alcohol Treatment Specialist.
A graduated student in The Addicted Brain
And more.
Thank you.
~Anon
Do you know what would be more than welcome?
A detailed criticism of specific points I made in this article.
Do you know what value I place on mudslinging from a person who won’t even attach their name to their mudslinging yet claim authority and imply an entitlement to be taken seriously? ZERO ZIP ZILCH 0 NADA. THAT’S HOW MUCH VALUE I PUT ON THAT.
You realize your like the one millionth person to come here and try to verbally abuse and shame me without ever lodging a single damn substantial criticism of a single point that I made, right? You’re comments are completely useless.
Here’s you: “duuuuhhhhhhhh, I’m a neuroscientist and you’re a jerk, so you’re wrong because I said so and I went to a university, addddoooooooiiiiiiiiiiiiiiiiiii.”
Here’s me: “Your comments have no scientific content whatsoever.”
Bring it, or shut up. You are wasting everyone’s time.
-Steven Slate (my NAME that I attach to MY WORDS, that have SUBSTANCE, instead of VACUOUS MUDSLINGING)
Nobody gives a shit about what you value, because it’s just shit.
You sparked a little anger from ol’ Steven, Anon! Good on you! It’s about time someone with some sense posted here. And this is one for you Steven…..it doesn’t take science to prove that your theory is wrong. Ask any addict who has real-life experience with the affliction, it’s obvious from your “copy and paste” logic that you could never truly relate. The only addiction you suffer from is always having to be right.
I’m an addict with real life experience in addiction and I believe Stevens article to be spot on. Believing in some self defeating excuse that addiction is a disease never helped me or the people who cared about me. If addiction is ruining your life or those of others then do something about it. It’s that simple but not easy. If you need to seek help them do but at the end of the day it’s you that overcomes the addiction. You are stronger than the addiction, it just takes time to learn and believe that. You aren’t a bad person because you fell into the trap of addiction but it’s also not a disease that you are powerless over.
Also, Steven. I do not know you. I can understand that you made a mistake. Humans make mistakes, Steven. I apologize that you can also not handle the truth, obviously. I can see by reading just a few comments above. Now, Recommending Saint Jude Retreats and saying, “Go detox.” Clearly shows that you also have no personal experience. Psychology is “NOT A SPECTATOR SPORT”. I hope you know who said that. Surely, you do, considering you already “know” so much, Steven.
Sincerely,
That Duke Student
~Anon
A neuroscientist? From where? Wal-Mart U? There’s a helluva lot more to addiction than science. Obviously you missed that day in school. You have no real world experience, and I sincerely doubt you have experienced what addicts go through…..you haven’t a clue. You stand behind your website and preach, belittling anyone who challenges you. You can’t stand it when someone finds fault in your “research”, and use science as your proof, and then make asinine comments about people not making scientific claims to debunk yours. Get off your high horse Steven and walk in the shoes of a true addict, if you survive. Anon is right on the money, and you’re short about 5 gagillion dollars.
I really can’t believe the nonsense I have to deal with here.
HE came here to tell me that he studied neuroscience and that I am wrong.
Then he offered literally no explanation of why I am wrong on the grounds he claimed to have authority on.
I am not just randomly asking someone for a scientific explanation of why I am wrong. Do you get that? He claimed authority in that field and claimed that I am wrong. I am simply asking him to make some reasonable attempt to back up his claim. I have backed up mine.
It never stops.
Oh and I am a recovering addict as well. I took my own initiative to study this subject and several other subjects. In fact I was addict for several years, on the streets and all.
So thank you so much. But, I have more than you know in REAL WORLD experience.
~Anon
That Duke Student
Studied neuroscience my ass. Give some proof that you studied this at university. I have a doctorate in neuroscience from the university of Cape Town. I too am a recovered addict and have dedicated my life to using neuroscience to understand addiction. It’s my conclusion that addiction isn’t a disease. Anon you are wrong because I’m more qualified then you and I say it’s not a disease.
Grow up
Hmmm, just from reading these comments it seems that the addicts (or recovering addicts) say it is a disease, thereby giving them a total out for ANY responsibility for their behavior. You have the people who study addiction but have never been an addict, saying it’s a disease, although they have nothing to base it on except people who are addicts or are recovering addicts claiming they had no choice, so it must be true. Then there are those of us who grew up in the 60’s, we know the truth kids, been there, done the drugs. This generation of kids have been raised to think that nothing is their fault and that there are no consequences to their actions, and when they do screw up it is everyone and everything else’s fault but theirs. Grow up, take responsibility for your CHOICES and that is exactly what drugs are, a CHOICE. Heard every excuse in the book from my kid and they were all crap. If you don’t start, you don’t get addicted plain and simple. I just see a bunch of cry babies looking for sympathy for destroying their lives and the lives of the people around them. And for all you “scientific” types, why not put all your collective brains together and try to find a cure for the real diseases like childhood cancer, diabetes, Alzheimer’s, MS, and Parkinson’s. Those are the people who had no choice in their REAL diseases.
I came here on accident, actually. I shouldn’t have to point out every single thing that is wrong with this forum or article, whatever you may call it. You should just do your own research. By the way, that’s actually not a way to “not take responsibility” in fact, there are several people who do not realize that it is a disease, addicts included. What about prescription medication addictions in elderly people? I’m sure they CHOSE to become addicted. Your brain actually searches for and yearns for missing chemicals in the brain. A pregnant woman will eat dirt if lacking in something found in the dirt. I’m sorry I do not have the time to show you how ignorant you people are. I sincerely apologize.
~Anon
Oh, and ANON is a female.
-That Duke Student.
Oh, LJ Sharpe. I am a mother as well. MY mother watched me struggle with this affliction. If you understood this illness you would understand that by “risk factors” we simply mean, “RISK factors” not “DISEASE FACTORS”. Let me break it down for you.
If you have a 12 year old child right? (Studies from SAMHSA show that children exposed to drugs at an earlier age, ‘around 12 years old’ seem to have a higher “RISK” for addiction and the prevalence of drug dependence from 12 year olds is 22.73% vs. around the age of 20 being around 6.49%) Then this adds to her case as a “risk factor” now. This would NOT typically be a “risk factor” for a 20 year old. Now, we are going to add a few more “risk factors” to this 12 year old girl’s case, alright? Follow along, now.
Availability of drugs. Meaning, these drugs are available to this child, she is unknowingly exposed to this drug. Her parents do it, her family does it, etc.
Now, let’s add stress to the mix. These parents fight ALL the time, domestic abuse is common in drug abusers.
This little girl (for argument’s sake guys) tries this drug because of ANOTHER “risk factor” peer pressure.
OR, this little girl is FED this drug by family members.
Whichever you prefer. In this case, it IS NOT a choice.
For example, if this SAME LITTLE GIRL, (let’s take away drugs) is exposed to a sexual situation at 12, from a member of her family, peer group, etc. With some risk factors like, stress, coaching, etc.
She participates in a sexual situation with this.
OR, is forced into it.
BUT, is this her fault?
I didn’t think so.
Also, let’s say that this little girl chose to STOP DOING DRUGS or NEVER TOUCH THEM AT ALL, but, 10 years later becomes an addict. IF you’re smart you can figure out what has changed in this little girl to make her think this is a solution, or EVEN IF SHE JUST WANTS TO DO IT.
WHY does she want to do it?
Because she was exposed, stressed out and many other factors.
Now, your case, I can see a few scenarios.
1. You were not raised by your parents.
2. If you were, your whole life, and they struggled with addiction, they caused a mark on you to where you are simply afraid to do drugs. It plays a ROLE that your SON is an ADDICT. Apparently, you do NOT understand genetics. Because you just gave me that one. No need to comment there, I hope. (Is it possible, for diseases to skip generations? emphatically, yes.) I am also going to emphasize what I meant by risk factors not completely determining an addict, (like you) they, I repeat, DO NOT DETERMINE INDEFINIETLY WHETHER OR NOT YOU ARE AN ADDICT)
I will agree with you on one thing, that addicts use this as a cop out, most have cop out methods because of this affliction. If you understood addiction, you would know this.
Actually, I’m not going to play out all of my scenarios but consider yourself blessed, and with that ‘holier than thou’ attitude, you gained an addict son, congratulations.
What role did you play in HIS life? It’s always his fault isn’t it? So there’s a little ping of guilt in your heart?
So you AID his addiction, or PAY for his treatment, when you know he will go back. Unknowingly supporting the addict in him ALL along. Or worse, LJ, you don’t help your son at all, and he gets angry (textbook) and he steals from you. Because you DO NOT KNOW obviously, how addiction works scientifically, personally or the like. There are several professors that compare addiction to HEART DISEASE and other diseases for people like you, I’d research them. And instead of being on this site with your petty life story of you and your family. Try learning something about it. Try HELPING your SON. Like for fuck’s sake woman get off your high horse. I know this will make you angry.
But, in all honesty, I’m not trying to make you angry. I only want you to understand.
And your son needs help.
I see everyone through sober eyes and I have for awhile. Do you know people with certain metal diseases are on an inward path of destruction due to the disease, and I’m not speaking on drugs right now.
But, you will still be blind and deaf and dumb. And you won’t see or listen or learn.
I hope that YOUR battle with cancer is successful and I wish you the best, because cancer is a B*TCH. Without question, LJ. But, it also can’t be YOUR cop-out on your son, you are still a mother, but hey. In your head, he’s probably too far gone, huh?
What I mean to say, is your strong enough to comment on this forum, like you did. But you aren’t strong enough to pull up a website and do some research.
http://www.drugs.gov
http://www.samhsa.gov
http://www.niaa.nih.gov
Here’s some sites for you all to check out. Or don’t, it doesn’t affect my life any, TRUST ME.
~ANON
(That Duke Student again)
Here’s an experiment for this study:
Control group: healthy brain scan
Then you scan the brain of an active, hardcore heroin addict. Then make them stay clean for a week, scan their brain, then a month, scan their brain, if they’re still alive past that, find another heroin addict. It shouldn’t take long to find one that will be dead well within a month.
Maybe these studies don’t recognize minor addictions as a brain disease, but physical dependence upon a substance cannot be defined otherwise! Opioids, especially ones on the more hardcore extreme of the spectrum, are some of the most addictive, dangerous substances on planet earth. Heroin, morphine, and other extremely potent, addictive drugs will create a physical dependence that cannot be escaped simply by just stopping use of a drug. When an individual is physically dependent upon a substance, they need to seek medical help so they can be eased out of the addiction, they cannot just abruptly stop taking it. If this organization is going to sit here and spew out that people can CHOOSE not to be addicted to something, people should be fully aware of the huge load of bullshit that is. I can’t choose to stop utilizing oxygen as an organism, similarly, a heroin addict can’t choose to not be addicted to heroin. It’s reminiscent of sexuality: a homosexual person can’t just CHOOSE to be heterosexual, that just is not who they are. Once an individual has reached the point where they are physically dependent upon the use of a substance, it is not just a choice to become not addicted. That individual can’t just go back to normal life, they need to seek out medical help, they need to be treated and freed from oppression. I know an individual who is addicted to heroin, and they have tried to be clean, but they can not stop abusing heroin. They have been to some of the most prestigious drug abuse centers in the world seeking help, but they are completely physically dependent upon this drug, and it is not their choice to just stop. Maybe this orginization needs to take into consideration that physical dependence is something that people face.
I think the debate is a healthy one. I was an addiction counselor for about 10 years. Attended the Johnson Institute (back in the 80’s) and they are a big proponents of the disease model. I stopped drinking when I was 26, went to AA meetings, did the steps. I was drinking close to two bottles of wine a night when I quit. I also had done a fair amount of hard core drugs, but they scared me so I didn’t continue using drugs. Quitting was easy. I stayed in AA for 5 years. I ended up not liking the AA rhetoric so continued to stay clean for another 7 or so years without AA. It wasn’t difficult. I decided to try drinking moderately, and I can tell you today, I have been successful. I have been a social drinker with no issues or problematic consequences for the last 18 years. I have an extremely happy and productive life.
For me, the disease model is a tool for people to use. I think the medical industry cannot answer this one, or at least it hasn’t so far. And for the average person, I’m not sure it matters. With that premise, perhaps we can let go of the anger and attacks (on Steve and others). People have the right to explore and think, and decide for themselves. If you relate to the disease model and it helps you quit then that’s great. In my experience, people DO quit on their own, and they can learn to drink responsibly. Others try and fail multiple times. Some get into recovery then die of lung cancer because they couldn’t stop smoking tobacco. Addiction is a horrible life, whatever the cause, get help, and find that your life will be better.
What a fantastic comment. Thanks for sharing what you’ve done and seen and thought about the whole thing. Much appreciated.
If you’ve read through the site, you might’ve noticed my position is basically this: that no matter what people say about what fuels their “recovery”, at the core, they all did it the same way: by authentically realizing they’d be happier with less/no substance use, and then simply doing that. They may credit counselors, sponsors, higher powers, support groups, books, pills, treatments, rock bottom experiences, or whatever, but I think that at the end of the day they just finally came to that realization at their core. In the meantime, we have narratives about recovery that comfort us, and they often involve attributing our change to something outside ourselves.
I also feel that the answer between “disease” and “choice” is probably somewhere in between. Since the body and brain are constantly adapting, it certainly seems probable that there are brain changes that occur in the reward / decision making functions that make choice more difficult for someone that has abused substances. Choice is not then impossible, as people are not compelled to use, but simply more difficult. The normal brain functions become somewhat diminished by the constant barrage of substances, but not destroyed. Choice in normal terms is compromised but not to the degree that it is impossible to choose.
craving does seem like a real experience and this could possibly be due to changes in the reward system. It certainly is possible/probable that the brain responds to massive releases of dopamine by reducing it’s natural output, leaving a person quitting meth for example with below average output for a period of time until the brain adapts again. If natural dopamine output is reduced, this could lead to craving the drug that releases dopamine to feel normal.
If all activities seem to affect the brain in some way, we might say that some activities result in changes to the brain that produce behaviors that we consider neutral, some in activities we consider positive, and some (like substance abuse) result in brain changes that we consider negative.
I think you had a milder form of alcohol abuse. I think you used abstinence for a sufficient amount of time and then could become a moderate drinker. Congratulations. What I don’t think is possible is severe problem drinkers or users moderating without a period of abstinence.
After much reading and research I’ve gain a much greater understanding of all the “jargon”….. as Steven call it. The terms addiction and disease are really not a total picture. There is alcohol use, alcohol abuse and alcoholism…. as there is drug or substance use, substance abuse and chemical dependence. Across the board alcoholism and chemical dependence are considered medical problems, conditions or diseases, depending on the terms one chooses to use. I do believe people who use or abuse alcohol or drugs can make a choice to stop or use less. Some people do it on there own, some use self-help meeting and some seek more intense treatment. Some choose moderation or abstinence. Once you have alcoholism and chemical dependence your in a whole different area with a whole different set of issues and problems, medically, physically, psychologically, socially etc. And just as different levels of treatment works for users and abusers, different intensities of intervention and treatment are needed for alcoholism and chemical dependence. These change your brain and body and one will always be at risk of harm if an alcoholic continues to drink and the chemical dependent continues to use. Can they safely choose moderation? That’s really high risk behavior because just like once you get lung cancer…. one or two cigarettes a day really isn’t helping you at all. The binge drinking college student has a choice…. are they at risk of dying of alcohol poisoning? Yep. Do they go through withdrawal? They sure can. The risks to an alcoholic, what they can die from, (cirrhosis, organ failure, acute withdrawal), is a whole lot different with a much greater risk. The chemical dependent has also undergone severe changes in the body and brain. So the theories, thoughts and beliefs on The Clean Slate make sense until that line of alcoholism and chemical dependence has been crossed.
Here’s what I’m thinking. The brain is an organ. We also know that the brain adapts/changes in response to any number of inputs, including of course taking substances. We also know that brain seems to be compartmentalized, i.e. different parts of the brain perform different functions.
Isn’t it probable that heavy substance abuse can cause the brain to adapt to the onslaught of chemicals to such a degree that the functioning of that section of the organ is compromised or damaged? If the organ is damaged, and the result is that it functions at less than full or normal capacity, then by definition I think we would call that a brain disease. In any other part of the body, an organ that is not functioning properly would be called a disease. Why not the organ of the brain? Isn’t it possible/probable that it can be damaged just like all other organs of the body? Even if the brain is only temporarily damaged, i.e. can repair itself to full or close to full capacity over time, that doesn’t mean that at one point it wasn’t diseased.
We already know through MRI’s that the brains of a substance abuser look different from a normal brain. We know for a fact the brain has adapted in some way. What we don’t know, and I believe the limit of our scientific knowledge is the cause, is if that adaption compromising the functioning of the brain in a negative way such that we would say the organ is damaged or compromised. A damaged organ where functioning is impaired I think we would classify as a disease. If that organ is the brain, a brain disease.
If substances do damage the areas of the brain that are responsible for reward/motivation and /or decision making, then we would expect that the impaired functioning of reward seeking and decision making would be a symptom of a diseased brain. In other words, if you damage the part of the brain whose primary function is to make decisions, the symptom would show up as poor decision making. If we damage the section of the brain related to rewards/motivation, then the symptom of that damage would be impaired actions related to seeking rewarding behaviors.
How does this relate to the choice / brain disease question? First of all, impaired does not equal destroyed. An organ can function at some level less than optimum without being in a state where it is completely not functioning. So it seems possible to me that if a section of the brain related to decision making is damaged, but not destroyed, a person could have a harder time making decisions but it would not be impossible to make them. The fact that some people can choose to stop using doesn’t mean that no damage has been done to the brain area that controls choice. Choice may simply be compromised by brain disease, not obliterated. Choice then might be said to be more difficult but not impossible. This lands us solidly in both camps. No you don’t lose 100% of your ability to choose. You are not compelled to use drugs. But your ability to stop using them may still be compromised. Stopping then is simply more difficult, but not impossible. You have a brain disease which results in diminished choice.
Thoughts?
Having been in recovery from crystal meth for over 6 years and not believing 100% in the disease model, I do know from experience that some of the components of addiction and a general dismissal in comments and claims here are in direct correlation to the disease model. That sounds a little confusing, so let me explain. As far as addiction being of a organic/disease process, I find no evidence of that being so. But addiction is a multi-faceted and complex issue with underlying causes other than an actual disease process, whether it be physical, emotional or mental. It is interesting to note that while one person can use a drug and not have it become habitual is different for others. I believe there are factors, and it doesn’t have to be physical that can make one person more susceptible to the throws of addiction. In contrast to what is stated here, there is an undefined threshold or line for some individuals that once crossed, there’s no turning back. Those who do not become addicts or alcoholics, for some unknown reason cross that line or threshold, and don’t have the compulsion to do it again, or they may be able to pick it up and put it down at will. All the scans and scientific data in the world can’t definitively say why subject A continues down a path of destruction and subject B seems “perfectly normal”.
I am certainly not a scientific expert on addiction, or any other subject for that matter. What I am is a person who used alcohol and drugs for a very long time, and as long I remained in the active usage status, I had no self-control over how much I used, when and for how long. I’ve read a lot of comments here that are pretty biased, and by that I mean that the experience of one, or several people can not be used as a “blanket” explanation for everyone. I don’t believe there’s one person here that can say they know exactly what another person’s experiences are like, and because something worked for them, it will work for anyone else. It’s simply not the case. That being said, I can’t say for certain that when a person says they had the willpower to put down the drug or alcohol and stop cold-turkey is not true. If you can do that, my hat’s off to you. It’s not the case for most of us. I did choose of free will to pick up my drink or ingest drugs for the first time, and it wasn’t until many years later that one day it came to me, I’m an addict….and that’s a broad description because, at least for me, being an addict doesn’t have to define whether it’s alcohol or drugs, or any other form of addiction.
For many addicts, claiming to have a disease and use it as an excuse for their behavior, continued use and proliferated destruction of their lives and of those around them, is just that, an excuse. The compulsion to keep using is real, not imagined or something that can be turned off by a switch. This is where I disagree with some of the claims here. The analogy of the taxi-driver and an addict’s neurological pathways is, in my opinion, a poor one. Let’s assume that the taxi-driver is a social drinker, he drives around London, and his brain builds those pathways of remembrance, and before you know it, he doesn’t need maps anymore. The addict uses a drug, and a pathway is paved as well. There’s one main difference: Being a taxi-driver and the “modified” brain behavior that occurs over time doesn’t have any sense of reward associated with it. Well, perhaps with the exception of feeling good about knowing all the shortcuts around town. The addict’s reaction to the drug far surpasses any reward system the taxi-driver receives…..which is why this analogy is obviously flawed. The rapid increase and decrease of brain chemicals such as dopamine and serotonin, and the emotional reaction to that fluctuation are what I believe compels an addict to continually seek out and creates a cycle of drug use and proliferation.
It’s easy for someone who hasn’t had a real issue with drugs or alcohol to interpret the addict’s response to the disease model as being an excuse. First off, an addict deep in their active addiction will take that information and make it apply to them. And since an actively using addict will find any reason to justify their using and continued use, this disease theory is something they can latch onto and go with. There are also those addicts who have been sober for some time and subscribe to this theory. The difference between them and the active using addict is that the sober person takes action to change behavior, and makes wrongs done in their past, right. It’s clear that someone who is still using drugs and someone who’s not can’t make that distinction. It’s only right that someone not in their right mind can use the disease model to their advantage, and not only until they reach a point when a moment of clarity comes upon them, that they can start to take action to change their lives.
The point I want to make here is not that you are wrong and I am right, far from it. I want to impress upon people who see a clear cut delineation of having willpower and not, is that it’s much more complex than that. There are so many factors involved, and each case is unique, albeit there are more commonalties than not. What occurs with one individual is not at all indicative of another. While there are many similar circumstances, each has to be assessed as individual and not clumped into a “general file”. I don’t think it’s a matter of not being compassionate, caring or understanding. It’s a matter of empathy….taken to the limit of it’s definition and just not having a general understanding of a person’s emotions, feelings or experiences. It’s really a matter of having walked in their shoes, lived their lives and experiences, and the consequences they face as a result of those experiences and consequences. From my own personal experience in being sober for over 6 years, when an addict is met with hostility and treated like an outcast, why would they want to help themselves? Being told that they’re bad, a social deviant and they don’t amount to anything is one reason why for so many addicts they stay in their addiction. This is certainly not indicative of every addict, there are always exceptions to every rule or situation. I don’t see any indication, at least in my circle of recovery, that we wanted to be treated as babies, coddled or held, and given special privileges and concessions. And I certainly don’t see anyone who uses the disease model as an excuse for past behavior, instead not using it as a crutch, and then as a tool to effect real and positive change in their lives.
Steven, I really thought long and hard about posting this since I have a reputation of being somewhat of a whiner, disputing your claims and responding with ill-informed responses and comments. What I posted today did not require me to research or Google anything. It is from my heart, and presented as from my personal experience. As I stated before, I am not a scientist or professional research kind of guy. My only intention is to present this as an adjunct, or an alternative way to view your already well researched and scientific data. What it is “not”, is to defame or discredit. Thanks!
Lets take alcohol to make it simple. We know over time that alcohol damages the liver and the hearts. Damage isn’t the same as destroyed, they can keep working up to a point for a long time even though damage has occurred. But they aren’t functioning at 100% or in a normal way.
So just about everyone acknowledges that over time alcohol abuse will damage organs such as the liver and heart. But it’s an incorrect assumption to think that alcohol abuse might also damage (but not destroy) the organ called the brain?
In order to argue against the brain disease theory, you have to believe that while we know for a fact that alcohol damages the liver and the heart, it is impossible that alcohol also does damage to the organ called the brain. It damages the liver, damages the heart, but leaves the brain alone and undamaged? Is that reasonable?
I think confusion comes because people confuse damage with destruction. Your liver can be damaged and still continue to function on a level. So can your heart be damaged and continue to function at less than optimal rates. Isn’t it also at least possible that your brain can be damaged, continue to function, but at less than optimal rate?
I agree that there needs to definitely be changes to a person with addictions life, however this article suggests that addicts are stupid idiots that just choose to ruin their lives. Leave loved ones and lose jobs because they are stupid idiots. They would have to be. Who else would choose to drink or drug their lives away other than idiots? No one can deny that some people react to drugs and alcohol differently. Other wise why would educated people decide to ruin their lives. Good christian, and other religious people suffer from this illness. It was also said that treatment center’s don’t help people. After d tox people need to learn tools as to how to live life on life’s terms. For decades people have polluted themselves and therefore avoid all feelings and activity’s of daily living. How can these people all of a sudden grow up and live sober with out help. The writer of this article is heartless and uneducated. Wake up.
I believe who ever wrote or all of you that believe the bullshit that you can control it needs to watch this video! and im not a alcohol or drug user
https://www.youtube.com/watch?v=qjyvRQFbseQ
I married an addict many years ago. I did not know he was as I was partying at the time too. When I stopped doing , he did not. As the years wore on I saw how when he was upset with something or he was “triggered” he would do drugs. He CHOSE to do drugs when he was upset instead of talking about things. We also ran social housing and AA was a big part of their recovery. I would be sickened to my stomach watching these people USE people so they could get money or food because they spent their money on drugs. I witnessed when my husband got clean how in the AA meetings, they would go on how the addiction was not their fault and they were powerless. For over 15 years I saw how they thought they made themselves “special” and “unique” that they were different from the rest of society so you would keep coming back. Notice you have to put money in a basket that they pass around? Because no government will support a program such as Alcoholics Anonymous that the recovery rate is between 5 and 10 per cent. Proven to be the WORST in all of medicine. I got tired of the enabling of the AA program and tired of the message that enabled people to feel sorry for themselves and saw the the suffering of children and adults who did NOT do drugs. The were dying of leukemia and cancer through no choice of their own. They were Suffering because they had a REAL disease. They did not pick up a needle and inject themselves with their disease. They did NOTHING TO THEMSELVES. And each person would have done ANYTHING to live. If a doctor walked in and said you stop eating apples and you will live they would do it. Addicts have choice. Walk through a children’s hospital and try to say otherwise. I would love to put an drug addict in a bed placed next to a 6 year old dying of leukemia. This article is exactly right. But no matter what addicts who enable themselves will read this and guffaw. They will always say 1+1 is 5 because they NEED it to be. They will always say they have no choice. The reason being after being around addicts for so long, is so they do not have to look at what they really do. Pure and simple. They get to enable themselves and not be fully responsible. When you have to take responsibility for your actions, FULL responsibility. Drug addiction is just that. ANOTHER FORM OF ADDICTION. Just like food or shopping. But its drugs. Plain and simple. I don’t support AA because I have seen the destructive behavior this program teaches. To each their own on what they do for their recovery but Im not concerned what an adult chooses to do with their life. Grown ups need to take responsibility for what they do. The world would be a lot better place if addicts took full responsibility. Kudos to those in the comments who did that. You just make the world a better place. And those who want to enable themselves and say they have a disease….Karla the 7 year old in bed 5 with Acute Lymphocytic Leukemia says hi.
Whether you are a true addict/alcoholic or not (which you actually may not be due to your beliefs on this), something tells me that you tried a 12 step program but couldn’t stand taking a look at yourself and all of your character defects. So, you resorted to hiding behind intellectualism and a computer screen, writing this article and responding to comments with such anger and bitterness. You poor thing.
I think the one main issue that most people have with this article is not so much the content, but the way it’s presented. There’s a lot of scientific data, charts and graphs, statistical information and of course, testimony from people with their personal experiences. I’ve been a thorn in Steven’s side for a few years, and my comments and contributions have not always been welcome. Most of the recent comments that I’ve read all seem to say pretty much the same thing…..the condescending tone towards addicts who don’t fit the “blanket” notion that anyone can stop on willpower alone, and insinuations that they are weak and less-=than. My congratulations to those who choose to stop by making what was for them, a simple choice. The fact of the matter is, and the video that Miranda posted explicitly explains why for most addicts or alcoholics, it’s the lack of choice that addicts have, and cannot simply be attributed to a lack of willpower. There is one small part of this article that I agree with, and that is that the brain forms pathways of habit, and those pathways can be “trained” to do something different. But again, willpower has absolutely nothing to do with the start of that process. An addict or alcoholic has to reach a point of no return, or as 12 steppers call it, hit a bottom. Some of those bottoms are higher than others, and trying to compare one to another is like saying because one person is a good driver than another, or, not relevant. Everyone is different, which is where I find fault with some of the material presented here. It does not take into account the experience of the individual, what works for one doesn’t always work for another. After years of being sober, reading comments here and doing my own research, I can’t completely wrap my head around the disease model. I personally feel that addiction in it’s worst case, does cause disease processes. In some way, maybe addiction is a disease because it is a root cause of diseases that ensue as a result of continued use. It’s a grey area for me.
I don’t think people who use 12 step programs as a program of recovery are brainwashed or coerced, some drink more Kool-Aid than others. It has worked for thousands upon thousands of people, and each takes from it what they need and what works for them. One of the main components of 12 step is the concept of Spirituality, not a crutch, not an excuse, but something outside of and bigger than oneself. I used for more reasons that Carter has pills, but for me, and this is very personal, it the root cause of my addiction was due to a Spiritual malady, or in other words, I had nothing to believe in. It’s not religion, cult or cop-out, but more a personal and unique experience. The reasons addicts use are similar from one to another, but, their experience in recovery, while on the outside looks similar, is completely unique. Science explains a lot, but it’s the unexplained things that this article doesn’t take into account when making blanket statements, and is as perceived by many that read it, biased, negative, and utterly and completely discounts personal experience. Thanks!
This right here that you said is key:
It ALWAYS comes back to reasons. People speak of disease as if there is a faulty brain mechanistically pushing them to want drugs, yet right after saying that, they start talking about the “reasons” they use – it helps with trauma, depression, anxiety, I’m lonely and it’s the only way I feel good, etc etc etc etc etc. Why all the reasons if it’s mysterious neurologically determined behavior???
Because it’s not a disease, it’s basic human behavior. It is people making choices that they think will meet the ends they’re trying to achieve.
Another thing Clay. You said this:
I have made great pains over the years to stress the point that I do not think this is a matter of willpower. In fact, in this very article I added a paragraph years ago to make that point. Here it is:
Yet people keep popping onto this page and arguing against a claim that I HAVE NEVER MADE: that this is about willpower. It is not. It is about will – i.e. preference, wants, or what one thinks will serve their purposes/help them achieve their ends. “Addicts” are simply people who believe heavy substance use is their best currently feasible way to get what they want – happiness, stress & depression relief – whatever they think it does for them that they believe they have no better means of achieving. It’s not that they’re weak – they are strongly pursuing what they think they need at the time. Trust me, I’ve been there, I’ve literally walked 13 miles in a snowstorm to shoplift, sell my stolen goods, and then buy heroin. That was a display of strength. I strongly pursued my will, which was to get heroin.
Another point, and really, I’ve been covering it right in that paragraph. I have also tried to explain that there are all kinds of choices in this life and that they aren’t all “simple.” Here’s a lengthy excerpt from an article I posted in 2014. Hopefully you’ll read it and STOP ARGUING AGAINST A STRAWMAN:
Best Wishes
-Steven Slate
The article implies changes to the brain due to substance abuse are “normal” That does not mean they are beneficial. Changes to the heart, the kidneys, and liver due to alcohol abuse are also “normal” too as in we expect them to happen, but that doesn’t mean they aren’t damaging.
It’s absurd to think that alcohol and other drugs damage organs such as the heart, kidneys and liver, but by some miracle don’t damage the organ of the brain. If you want to say the damage that occurs due to substance abuse is normal, as in it is to be expected, fine. If you want to say that substances don’t damage the brain in a way that makes quitting more difficult, although certainly not impossible, I disagree.
You’re lumping cellular brain damage that results from toxicity together with neural adaptations that regularly accompany habit creation. One could rightly be called brain damage, the other could not. These distinctions are tough to weed through, and I don’t personally claim to know them all. But others including neuroscientists have confirmed some of my basic claims here. Actually, Nora Volkow’s own work confirms some of my claims here.
I do not believe there is satisfactory evidence which shows that brain damage that may occur as a result of substance use makes quitting particularly harder than any other activity in one’s life. Furthermore, the evidence shows that “addiction” extremely rarely fulfills the definition of “chronic” if at all – the vast majority of “addicts” eventually quit, moderate, change. It’s the norm. Look up Addiction and Choice: Theory and New Data (Heyman 2013) for a quick rundown of the evidence of that. It’s available free online.