

They’re screaming it from the rooftops: “addiction is a disease, and you can’t stop it without medical treatment”! But why are they screaming it so loud, why are they browbeating us about it, why is it always mentioned with a qualifier? You don’t hear people constantly referring to cancer as “the disease of cancer” – it’s just “cancer”, because it’s obvious that cancer is a disease, it’s been conclusively proven that the symptoms of cancer can’t be directly stopped with mere choices – therefore no qualifier is needed. On the other hand, addiction to drugs and alcohol is not obviously a disease, and to call it such we must either overlook the major gaps in the disease argument, or we must completely redefine the term “disease.” Here we will analyze a few key points and show that what we call addiction doesn’t pass muster as a real disease.
Real Diseases versus The Disease Concept or Theory of Drug Addiction
In a true disease, some part of the body is in a state of abnormal physiological functioning, and this causes the undesirable symptoms. In the case of cancer, it would be mutated cells which we point to as evidence of a physiological abnormality, in diabetes we can point to low insulin production or cells which fail to use insulin properly as the physiological abnormality which create the harmful symptoms. If a person has either of these diseases, they cannot directly choose to stop their symptoms or directly choose to stop the abnormal physiological functioning which creates the symptoms. They can only choose to stop the physiological abnormality indirectly, by the application of medical treatment, and in the case of diabetes, dietetic measures may also indirectly halt the symptoms as well (but such measures are not a cure so much as a lifestyle adjustment necessitated by permanent physiological malfunction).
 In addiction, there is no such physiological malfunction. The best physical evidence put forward by the disease proponents falls totally flat on the measure of representing a physiological malfunction. This evidence is the much touted brain scan[1]. The organization responsible for putting forth these brain scans, the National Institute on Drug Abuse and Addiction (NIDA), defines addiction in this way:
In addiction, there is no such physiological malfunction. The best physical evidence put forward by the disease proponents falls totally flat on the measure of representing a physiological malfunction. This evidence is the much touted brain scan[1]. The organization responsible for putting forth these brain scans, the National Institute on Drug Abuse and Addiction (NIDA), defines addiction in this way:
Addiction is defined as a chronic relapsing brain disease that is characterized by compulsive drug seeking and use, despite harmful consequences. It is considered a brain disease because drugs change the brain – they change it’s structure and how it works. These brain changes can be long lasting, and can lead to the harmful behaviors seen in people who abuse drugs.
The NIDA is stating outright that the reason addiction is considered a disease is because of the brain changes evidenced by the brain scans they show us, and that these changes cause the behavior known as addiction, which they characterize as “compulsive drug seeking and use”. There are three major ways in which this case for the disease model falls apart:
- the changes in the brain which they show us are not abnormal at all
- people change their behavior IN SPITE OF the fact that their brain has changed in response to repeated substance use jump to section
- there is no evidence that the behavior of addicts is compulsive (compulsive meaning involuntary) (point two addresses this, as well as some other research that will be presented) jump to section
This all applies equally to “alcoholism” as well. If you’re looking for information on alcoholism, the same theories and logic discussed here are applicable; wherever you see the term addiction used on this site, it includes alcoholism.
Brain Changes In Addicts Are Not Abnormal, and Do Not Prove The Brain Disease Theory
On the first count – the changes in the brain evidenced by brain scans of heavy substance users (“addicts”) do not represent a malfunctioning brain. They are quite normal, as research into neuroplasticity has shown us. Whenever we practice doing or thinking anything enough, the brain changes – different regions and neuronal pathways are grown or strengthened, and new connections are made; various areas of the brain become more or less active depending upon how much you use them, and this becomes the norm in your brain – but it changes again as you adjust how much you use those brain regions depending on what you choose to think and do. This is a process which continues throughout life, there is nothing abnormal about it. Here, Sharon Begley describes neuroplasticity: [2]
The term refers to the brain’s recently discovered ability to change its structure and function, in particular by expanding or strengthening circuits that are used and by shrinking or weakening those that are rarely engaged. In its short history, the science of neuroplasticity has mostly documented brain changes that reflect physical experience and input from the outside world.
So, when the NIDA’s Nora Volkow and others show us changes in the brain of a substance user as compared to a non-substance user, this difference is not as novel as they make it out to be. They are showing us routine neuroplastic changes which every healthily functioning person’s brain goes through naturally. The phenomenon of brain changes isn’t isolated to “addicts” or anyone else with a so-called brain disease – non-addicted and non-depressed and non-[insert brain disease of the week here] people experience neural adaptations too. One poignant example was found in the brains of London taxi drivers, as Begley and Jeffrey Schwartz pointed out in The Mind and The Brain. [4]
Is Being A Good Taxi Driver A Disease?
A specific area of the brain’s hippocampus is associated with creating directional memories and a mental map of the environment. A team of researchers scanned the brains of London taxi drivers and compared their brains to non-taxi drivers. There was a very noticeable difference, not only between the drivers and non-drivers, but also between the more experienced and less experienced drivers:
There it was: the more years a man had been a taxi driver, the smaller the front of his hippocampus and the larger the posterior. “Length of time spent as a taxi driver correlated positively with volume in…the right posterior hippocampus,” found the scientists. Acquiring navigational skills causes a “redistribution of gray matter in the hippocampus” as a driver’s mental map of London grows larger and more detailed with experience. [4]
So, the longer you drive a cab in London (that is, the longer you exert the mental and physical effort to quickly find your way around one of the world’s toughest to navigate cities), the more your brain physically changes. And the longer you use drugs, the more your brain changes. And indeed, the longer and more intensely you apply yourself to any skill, thought, or activity – the more it will change your brain, and the more visible will be the differences between your brain and that of someone who hasn’t been focused on that particular skill. So, if we follow the logic of the NIDA, then London’s taxi drivers have a disease, which we’ll call taxi-ism, that forces them to drive taxis. But the new diseases wouldn’t stop there.
Learning to play the piano well will change your brain – and if you were to compare brain scans of a piano player to a non-piano player, you would find significant differences. Does this mean that piano playing is a disease called Pianoism? Learning a new language changes your brain, are bilingual people diseased? Athletes’ brains will change as a result of intensive practice – is playing tennis a disease? Are soccer players unable to walk into a sporting goods store without kicking every ball in sight? We could go on and on with examples, but the point is this – when you practice something, you get better at doing it, because your brain changes physiologically – and this is a normal process. If someone dedicated a large portion of their life to seeking and using drugs, and their brain didn’t change – then that would be a true abnormality. Something would be seriously wrong with their brain.
Its not just physical activity that changes our brains, thoughts alone can have a huge effect. What’s more, whether the brain changes or not, there is much research which shows that the brain is slave to the mind. As Begley points out elsewhere, thoughts alone can create the same brain activity that would come about by doing things[2]:
Using the brain scan called functional magnetic resonance imaging, the scientists pinpointed regions that were active during compassion meditation. In almost every case, the enhanced activity was greater in the monks’ brains than the novices’. Activity in the left prefrontal cortex (the seat of positive emotions such as happiness) swamped activity in the right prefrontal (site of negative emotions and anxiety), something never before seen from purely mental activity. A sprawling circuit that switches on at the sight of suffering also showed greater activity in the monks. So did regions responsible for planned movement, as if the monks’ brains were itching to go to the aid of those in distress.
So by simply practicing thinking about compassion, these monks made lasting changes in their brain activity. Purely mental activity can change the brain in physiologically significant ways. And to back up this fact we look again to the work of Dr Jeffrey Schwartz[3], who has taught OCD patients techniques to think their way out of obsessive thoughts. After exercising these thought practices, research showed that the brains of OCD patients looked no different than the brains of those who’d never had OCD. If you change your thoughts, you change your brain physically – and this is voluntary. This is outside the realm of disease, this shows a brain which changes as a matter of normality, and can change again, depending on what we practice choosing to think. There is nothing abnormal about a changing brain, and the type of changes we’re discussing aren’t necessarily permanent, as they are characterized to be in the brain disease model of addiction.
These brain change don’t need to be brought on by exposure to chemicals. Thoughts alone, are enough to rewire the very circuits of the human brain responsible for reward and other positive emotions that substance use and other supposedly “addictive” behaviors (“process addictions” such as sex, gambling, and shopping, etc.) are connected with.
The Stolen Concept of Neuroplasticity in the Brain Disease Model of Addiction
Those who claim that addiction is a brain disease readily admit that the brain changes in evidence are arrived at through repeated choices to use substances and focus on using substances. In this way, they are saying the disease is a product of routine neuroplastic processes. Then they go on to claim that such brain changes either can’t be remedied, or can only be remedied by outside means (medical treatment). When we break this down and look at it step by step, we see that the brain disease model rests on an argument similar to the “stolen concept”. A stolen concept argument is one in which the argument denies a fact on which it simultaneously rests. For example, the philosophical assertion that “reality is unknowable” rests on, or presumes that the speaker could know a fact of reality, it presumes that one could know that reality is unknowable – which of course one couldn’t, if reality truly was unknowable – so the statement “reality is unknowable” invalidates itself. Likewise, the brain disease proponents are essentially saying “neuroplastic processes create a state called addiction which cannot be changed by thoughts and choices” – this however is to some degree self-invalidating, because it depends on neuroplasticity while seeking to invalidate it. If neuroplasticity is involved, and is a valid explanation for how to become addicted, then we can’t act is if the same process doesn’t exist when it’s time to focus on getting un-addicted. That is, if the brain can be changed into the addicted state by thoughts and choices, then it can be further changed or changed back by thoughts and choices. Conditions which can be remedied by freely chosen thoughts and behaviors, don’t fit into the general understanding of disease. Ultimately, if addiction is a disease, then it’s a disease so fundamentally different than any other that it should probably have a completely different name that doesn’t imply all the things contained in the term “disease” – such as the idea that the “will” of the afflicted is irrelevant to whether the condition continues.
People change their addictive behavior in spite of the fact that their brain is changed – and they do so without medication or surgery (added 4/18/14)
In the discussion above, we looked at some analogous cases of brain changes to see just how routine and normal (i.e. not a physiological malfunction) such changes are. Now we’re going to look directly at the most popular neuroscientific research which purports to prove that these brain changes actually cause “uncontrolled” substance use (“addiction”).
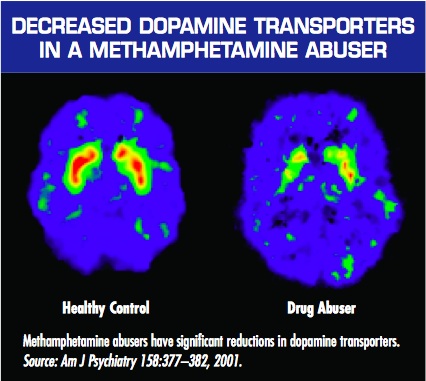
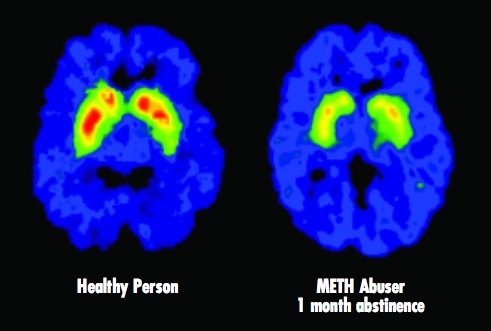
The most popular research is Nora Volkow’s brain scans of “meth addicts” presented by the NIDA. The logic is simple. We’re presented with the brain scan of a meth addict alongside the brain scan of a non-user, and we’re told that the decreased activity in the brain of the meth user (the lack of red in the “Drug Abuser” brain scan presented) is the cause of their “compulsive” methamphetamine use. Here’s how the National Institute on Drug Abuse (NIDA) explains the significance of these images in their booklet – Drugs, Brains, and Behavior: The Science of Addiction :
Just as we turn down the volume on a radio that is too loud, the brain adjusts to the overwhelming surges in dopamine (and other neurotransmitters) by producing less dopamine or by reducing the number of receptors that can receive signals. As a result, dopamine’s impact on the reward circuit of a drug abuser’s brain can become abnormally low, and the ability to experience any pleasure is reduced. This is why the abuser eventually feels flat, lifeless, and depressed, and is unable to enjoy things that previously brought them pleasure. Now, they need to take drugs just to try and bring their dopamine function back up to normal.
[emphasis added]
They go on that these same sorts of brain changes:
..may also lead to addiction, which can drive an abuser to seek out and take drugs compulsively. Drug addiction erodes a person’s self-control and ability to make sound decisions, while sending intense impulses to take drugs.
[emphasis added]
That image is shown when NIDA is vaguely explaining how brain changes are responsible for “addiction.” But later on, when they try to make a case for treating addiction as a brain disease, they show the following image, which tells a far different story if you understand more of the context than they choose to mention:
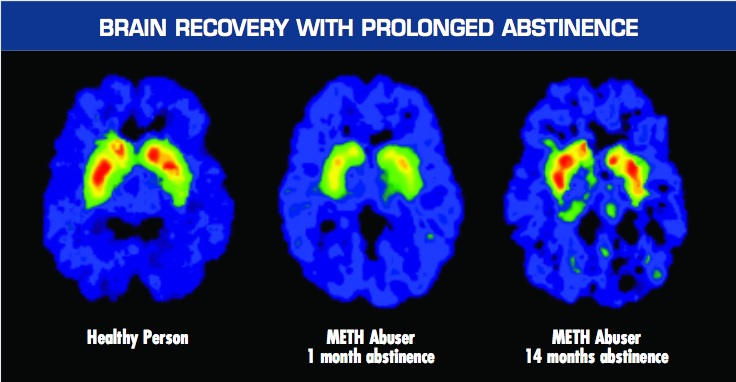
Again, this graphic is used to support the idea that we should treat addiction as a brain disease. However, the authors mistakenly let a big cat out of the bag with this one – because the brain wasn’t treated at all. Notice how the third image shows a brain in which the red level of activity has returned almost to normal after 14 months of abstinence. That’s wonderful – but it also means that the NIDA’s assertions that “Addiction means being unable to quit, even in the face of negative consequences”(LINK) and “It is considered a brain disease because drugs change the brain… These brain changes… can lead to the harmful behaviors seen in people who abuse drugs” are dead wrong.
When these studies were done, nobody was directly treating the brain of methamphetamine addicts. They were not giving them medication for it (there is no equivalent of methadone for speed users), and they weren’t sticking scalpels into the brains of these meth addicts, nor were they giving them shock treatment. So what did they do?
These methamphetamine addicts were court ordered into a treatment program (whose methodology wasn’t disclosed in the research) which likely consisted of a general mixture of group and individual counseling with 12-step meeting attendance. I can’t stress the significance of this enough: their brains were not medically treated. They talked to counselors. They faced a choice between jail and abstinence. They CHOSE abstinence (for at least 14 months!) – even while their brains had been changed in a way that we’re told robs them of the ability to choose to quit “even in the face of negative consequences.” [5]
Even with changed brains, people are capable of choosing to change their substance use habits. They choose to stop using drugs, and as the brain scans above demonstrate – their brain activity follows this choice. If the brain changes caused the substance using behavior, i.e. if it was the other way around, then a true medical intervention should have been needed – the brain would’ve needed to have changed first via external force (medicine or surgery) before abstinence was initiated. They literally wouldn’t have been able to stop for 14 months without a real physical/biological medical intervention. But they did…
Substance Use Is Not Compulsive, It Is A Choice
In his classic book Addiction & Opiates, Alfred R Lindesmith PhD explained the requirements of reliable scientific theories explaining the causes of things such as heroin addiction:
…a genuine theory that proposes to explain a given phenomenon by relating it to another phenomenon must, in the first place, have clear empirical implications which, if not fulfilled, negate the theory.
If the theory is that neural adaptations alone cause uncontrolled behavior, then this proposition can easily be shown to be false. I demonstrated above that in the midst of having fully “changed” or “addicted” brains, people do indeed stop using substances, so essentially, it is case closed. But the depths to which the brain disease theory of addiction can be negated go even further, because the basic theory of addiction as representing uncontrolled substance use has never been explained. Explanation of the mechanism by which substance use happens without the individual’s consent is conspicuously missing – yet such explanation is a necessary part of such a theory, as Lindesmith writes (again in Addiction & Opiates):
…besides identifying the two types of phenomenon that are allegedly interrelated, there must be a description of the processes or events that link them. In other words, besides affirming that something causes something else, it is necessary to indicate how the cause operates to produce the alleged effect.
“Here Comes the Bogey-Man” by Goya, circa 1799
There doesn’t seem to be any explanation or evidence that substance use is involuntary. In fact, the evidence, such as that presented above, shows the opposite. Nevertheless, when the case for the disease is presented, the idea that drug use is involuntary is taken for granted as true. No evidence is ever actually presented to support this premise, so there isn’t much to be knocked down here, except to make the point I made above – is a piano player fundamentally incapable of resisting playing the piano? They may love to play the piano, and want to do it often, they may even be obsessive about it, but it would be hard to say that at the sight of a piano they are involuntarily driven by their brain to push aside whatever else they need to do in order to play that piano.
There is another approach to the second claim though. We can look at the people who have subjectively claimed that their substance use is involuntary, and see if the offer of incentives results in changed behavior. Gene Heyman covered this in his landmark book, Addiction: A Disorder of Choice[3]. He recounts studies in which cocaine abusers were given traditional addiction counseling, and also offered vouchers which they could trade in for modest rewards such as movie tickets or sports equipment – if they proved through urine tests that they were abstaining from drug use. In the early stages of the study, 70% of those in the voucher program remained abstinent, while only 20% stayed abstinent in the control group which didn’t receive the incentive of the vouchers. This demonstrates that substance use is not in fact compulsive or involuntary, but that it is a matter of choice, because these “addicts” when presented with a clear and immediately rewarding alternative to substance use and incentive not to use, chose it. Furthermore, follow up studies showed that this led to long term changes. A full year after the program, the voucher group had double the success rate of those who received only counseling (80% to 40%, respectively). This ties back in to our first point that what you practice, you become good at. The cocaine abusers in the voucher group practiced replacing substance use with other activities, such as using the sports equipment or movie passes they gained as a direct consequence of abstaining from drug use – thus they made it a habit to find other ways of amusing themselves, this probably led to brain changes, and the new habits became the norm.
Long story short, there is no evidence presented to prove that substance use is compulsive. The only thing ever offered is subjective reports from drug users themselves that they “can’t stop”, and proclamations from treatment professionals that the behavior is compulsive due to brain changes. But if the promise of a ticket to the movies is enough to double the success rate of conventional addiction counseling, then it’s hard to say that substance users can’t control themselves. The reality is that they can control themselves, but they just happen to see substance use as the best option for happiness available to them at the times when they’re abusing substances. When they can see other options for happiness as more attractive (i.e. as promising a greater reward than substance use), attainable to them, and as taking an amount of effort they’re willing to expend – then they will absolutely choose those options instead of substance use, and will not struggle to “stay sober”, prevent relapse, practice self-control or self-regulation, or any other colloquialism for making a different choice. They will simply choose differently.
But wait… there’s more! (Added 4/21/14) Contrary to the claims that alcoholics and drug addicts literally lose control of their substance use, a great number of experiments have found that they are really in full control of themselves. Priming dose experiments have found that alcoholics are not triggered into uncontrollable craving after taking a drink. Here’s a link to the evidence and a deeper discussion of these findings: Do Addicts and Alcoholics Lose Control? Priming dose experiments of cocaine, crack, and methamphetamine users found that after being given a hit of their drug of choice (primed with a dose) they are capable of choosing a delayed reward rather than another hit of the drug.
Three Most Relevant Reasons Addiction Is Not A Disease
So to sum up, there are at least two significant reasons why the current brain disease theory of addiction is false.
- A disease involves physiological malfunction, the “proof” of brain changes shows no malfunction of the brain. These changes are indeed a normal part of how the brain works – not only in substance use, but in anything that we practice doing or thinking intensively. Brain changes occur as a matter of everyday life; the brain can be changed by the choice to think or behave differently; and the type of changes we’re talking about are not permanent.
- The very evidence used to demonstrate that addicts’ behavior is caused by brain changes also demonstrates that they change their behavior while their brain is changed, without a real medical intervention such as medication targeting the brain or surgical intervention in the brain – and that their brain changes back to normal AFTER they VOLITIONALLY change their behavior for a prolonged period of time
- Drug use in “addicts” is not compulsive. If it was truly compulsive, then offering a drug user tickets to the movies would not make a difference in whether they use or not – because this is an offer of a choice. Research shows that the offer of this choice leads to cessation of substance abuse. Furthermore, to clarify the point, if you offered a cancer patient movie tickets as a reward for ceasing to have a tumor – it would make no difference, it would not change his probability of recovery.
Addiction is NOT a disease, and it matters. This has huge implications for anyone struggling with a substance use habit.
References:
- 1) NIDA, Drugs Brains and Behavior: The Science of Addiction, sciofaddiction.pdf
- 2) Sharon Begley, Scans of Monks’ Brains Show Meditation Alters Structure, Functioning, Wall Street Journal, November 5, 2004; Page B1, http://psyphz.psych.wisc.edu/web/News/Meditation_Alters_Brain_WSJ_11-04.htm
- 3) Gene Heyman, Addiction: A Disorder of Choice, Harvard University Press, 2009
- 4) Sharon Begley and Jeffrey Schwartz, The Mind And The Brain, Harper Collins, 2002
- 5) Links to the 2 methamphetamine abuser studies by Nora Volkow:
http://www.jneurosci.org/cgi/content/full/21/23/9414
http://ajp.psychiatryonline.org/cgi/reprint/158/3/377
Important Notes from the author to readers and especially commenters:
On “badness” or immorality:
Please do not attribute to me the idea that heavy substance users must be “bad” or “immoral” if they are in fact in control of and choosing their behavior. I do not think this. I think that at the time they’re using, it is what they prefer, given what life options they believe are available to them – and I don’t think it’s my job to decide what other people should prefer for themselves, and then declare them bad if they don’t live up to my vision of a “good” life. That’s what the disease recovery culture does, de facto, when they present the false dichotomy of ‘diseased or bad’. To say that addiction is chosen behavior is simply to make a statement about whether the behavior is within the control of the individual – it is not a judgment of the morality of the behavior or the individual choosing it.
On willpower:
Please do not attribute to me the suggestion to “use willpower.” I have not said that people should use willpower, nor do I think it’s a coherent or relevant concept in any way, nor do I think “addicts lack willpower” or that those who recover have more willpower, nor, and this is important, do I believe that a choice model of addiction necessarily implies willpower as the solution.
“Addicts” do not need extra willpower, strength, or support, to change their heavy substance use habits if that is what they want to do. They need to change their preference for heavy substance use, rather than trying to fight that preference with supposed “willpower.”
On compassion:
Please don’t accuse me of not having compassion for people who have substance use problems. You do not know that, and if you attack my motives in this way it just shows your own intellectual impotence and sleaze. I have a great deal of compassion for people with these problems – I was once one such person. I am trying to get at the truth of the nature of addiction, so that the most people can be helped in the most effective way possible. I don’t doubt the compassion of those who believe addiction is a disease, and I hope you’ll give me the same benefit of the doubt. I assure you I care and want the best for people – and I don’t need to see them as diseased to do so. When you see someone who’s gotten themselves into a mess, don’t you want to help, even if it’s of their own making? Why should we need to believe they have a disease to help them if the mess is substance use related? I don’t get that requirement.
Some Agreement I’ve Found From Addiction Researchers (added 6/10/14)
I began working out my understanding of the brain disease model back in 2005 as I started working on a book about addiction; published this article in 2010; and was happy to find in 2011 when I went back to work with Baldwin Research that they had arrived at a similar conclusion. The way they stated it amounted to “either everything is addiction, or nothing is” – referring to the fact that the brain changes presented as proof of addiction being a brain disease are so routine as to indicate that all behavior must be classified as addiction if we follow the logic.
I was also gratified to have found a neuroscientist who arrived at the same conclusions. I think Marc Lewis PhD and I may disagree on a few things, but it seems we may see eye to eye on the logic I presented above about such brain changes being routine, and thus not indicative of disease. Check what he wrote in 2012 for the PLOS Blog, Mind The Brain:
every experience that has potent emotional content changes the NAC and its uptake of dopamine. Yet we wouldn’t want to call the excitement you get from the love of your life, or your fifth visit to Paris, a disease. The NAC is highly plastic. It has to be, so that we can pursue different rewards as we develop, right through childhood to the rest of the lifespan. In fact, each highly rewarding experience builds its own network of synapses in and around the NAC, and that network sends a signal to the midbrain: I’m anticipating x, so send up some dopamine, right now! That’s the case with romantic love, Paris, and heroin. During and after each of these experiences, that network of synapses gets strengthened: so the “specialization” of dopamine uptake is further increased. London just doesn’t do it for you anymore. It’s got to be Paris. Pot, wine, music…they don’t turn your crank so much; but cocaine sure does. Physical changes in the brain are its only way to learn, to remember, and to develop. But we wouldn’t want to call learning a disease.
….
In my view, addiction (whether to drugs, food, gambling, or whatever) doesn’t fit a specific physiological category. Rather, I see addiction as an extreme form of normality, if one can say such a thing. Perhaps more precisely: an extreme form of learning. No doubt addiction is a frightening, often horrible, state to endure, whether in oneself or in one’s loved ones. But that doesn’t make it a disease.
I think that quote is very important, because it highlights neuronal changes that occur in the same region implicated in addiction (whereas the examples I presented earlier in the article represented some other regions).
In a brilliant paper titled “The naked empress: Modern neuro science and the concept of addiction”, Peter Cohen of The Centre for Drug Research at University of Amsterdam, states that:
The notions of addiction transformed into the language of neurology as performed by authors like Volkov, Berridge, Gessa or De Vries are completely tautological.
He essentially argues that Volkow et al take for granted that heavy drug and alcohol use is uncontrolled, identify neural correlates, and present them as evidence of uncontrollability. Yet they don’t do so with other behaviors, and he provides plenty of examples. He notes that they start with assumptions that certain patterns of behavior (e.g. heavy drug use) are uncontrolled, and others are controlled – based purely on cultural prejudices. He accurately identifies addiction as a learned behavior, or as routine bonding to a thing, and then expresses something very close to my thesis presented above (that all learned/intensely repeated behaviors result in “brain changes”).
The problem of course is that probably all learning produces temporary or lasting ‘change in neural systems’. Also, continuation of learned behavior may be functional in the eyes and experience of the person but less so in the eyes of the outsider. Who is right? We know of people remaining married in spite of-in the eyes of a beholder- a very bad marriage. Who speaks of lasting ‘neural change’ as the basis of the continued marriage? But, even when a person herself sees some behavior as counter functional, it is not necessarily seen as addiction. It may be seen as impotence, ingrained habit or unhappy adaptation. It all depends on which behavior we discuss, not on the brain.
The great points contained in this article would be done an injustice if I tried to sum them up here, so check it out for yourself at The Center for Drug Research University of Amsterdam. As with Marc Lewis, I suspect that Peter Cohen and I might have some substantial disagreements about the full nature of addiction and human behavior in general, but I think we at least agree that the changes in the brain of an “addict” do not necessarily represent disease, and more likely represent a routine process.
Writing in 2013 for the journal Frontiers In Psychiatry, esteemed behavioral and addiction researcher Gene Heyman pointed out something so painfully obvious that we don’t even take notice – no causal link has ever been found between the neural adaptations caused by excessive substance use and continued heavy use. That is, correlation is not causation:
With the exception of alcohol, addictive drugs produce their biological and psychological changes by binding to specific receptor sites throughout the body. As self-administered drug doses greatly exceed the circulating levels of their natural analogs, persistent heavy drug use leads to structural and functional changes in the nervous system. It is widely – if not universally – assumed that these neural adaptations play a causal role in addiction. In support of this interpretation brain imaging studies often reveal differences between the brains of addicts and comparison groups (e.g., Volkow et al., 1997; Martin-Soelch et al., 2001) However, these studies are cross-sectional and the results are correlations. There are no published studies that establish a causal link between drug-induced neural adaptations and compulsive drug use or even a correlation between drug-induced neural changes and an increase in preference for an addictive drug.
Did you get that? Let me repeat the words of this experienced researcher, PhD, and lecturer/professor from Boston College and Harvard who, in addition to publishing scores of papers in peer reviewed medical journals has also had an entire book debunking the disease model of addiction by Harvard University press (I say all of this about his credentials so that I can hopefully STOP getting commenters who say “but you’re not a doctor, and what are your credentials wah, wah, wah,……” here’s a “credentialed” expert who essentially agrees with most of what I’ve written in this article – so please, for the love of god, save your fallacious ad hominems and appeals to authority for another day!)- he (Gene Heyman PhD) said this, as of 2013:
There are no published studies that establish a causal link between drug-induced neural adaptations and compulsive drug use or even a correlation between drug-induced neural changes and an increase in preference for an addictive drug.
And this was in a recently published paper in a section headed “But Drugs Change the Brain”, in which he continued to debunk the “brain changes cause addiction” argument by saying:
There are no published studies that establish a causal link between drug-induced neural adaptations and compulsive drug use or even a correlation between drug-induced neural changes and an increase in preference for an addictive drug. For example, in a frequently referred to animal study, Robinson et al. (2001) found dendritic changes in the striatum and the prefrontal cortex of rats who had self-administered cocaine. They concluded that this was a “recipe for addiction.” However, they did not evaluate whether their findings with rodents applied to humans, nor did they even test if the dendritic modifications had anything to do with changes in preference for cocaine in their rats. In principle then it is possible that the drug-induced neural changes play little or no role in the persistence of drug use. This is a testable hypothesis.
First, most addicts quit. Thus, drug-induced neural plasticity does not prevent quitting. Second, in follow-up studies, which tested Robinson et al.’s claims, there were no increases in preference for cocaine. For instance in a preference test that provided both cocaine and saccharin, rats preferred saccharin (Lenoir et al., 2007) even after they had consumed about three to four times more cocaine than the rats in the Robinson et al study, and even though the cocaine had induced motoric changes which have been interpreted as signs of the neural underpinnings of addiction (e.g., Robinson and Berridge, 2003). Third [an analysis of epidemiological studies] shows that the likelihood of remission was constant over time since the onset of dependence. Although this is a surprising result, it is not without precedent. In a longitudinal study of heroin addicts, Vaillant (1973) reports that the likelihood of going off drugs neither increased nor decreased over time (1973), and in a study with rats, Serge Ahmed and his colleagues (Cantin et al., 2010) report that the probability of switching from cocaine to saccharin (which was about 0.85) was independent of past cocaine consumption. Since drugs change the brain, these results suggest that the changes do not prevent quitting, and the slope of [an analysis of epidemiological studies] implies that drug-induced neural changes do not even decrease the likelihood of quitting drugs once dependence is in place.
Read the full paper here – it’s an amazingly concise summary of the truths about addiction that contradict many of the accepted opinions pushed by the recovery culture – Heyman, G. M. (2013). Addiction and Choice: Theory and New Data. Frontiers in Psychiatry, 4. doi:10.3389/fpsyt.2013.00031
Why Does It Matter Whether or Not Addiction Is A Brain Disease?
When we accept the unproven view that addiction and alcoholism are brain diseases, then it will lead us down a long, painful, costly, and pointless road of cycling in and out of ineffective treatment programs and 12 step meetings. You will waste a lot of time without finding a permanent solution. When we examine the evidence, throw out the false disease concepts, and think rationally about the problem we can see that addiction is really just a matter of choice. Knowing this, we can bypass the rehabs, and find the true solution within ourselves. You can choose to end your addiction. You can choose to improv your life. You can choose to stop the endless cycle of “recovery” and start living. You don’t need to be a victim of the self-fulfilling prophecy that is the brain disease model of addiction. There are alternative views and methods of change which I hope you’ll take the time to learn about on The Clean Slate Addiction Site.
There are many different ways to argue against the brain disease model of addiction. I have only presented 3 basic arguments here. But beyond just addiction, many modern claims of “brain disease” are fatally flawed, in that they are founded on the logically impossible philosophical stance of psychological determinism. From this standpoint, any evidence of any brain activity is immediately interpreted as a “cause” of a particular mind state or behavior – with no regard for free will/the ability to choose one’s thoughts and thus behaviors. If you understand the impossibility of psychological determinism (or “epiphenomenalism”) then you’ll take all such claims with a grain of salt. For a detailed examination of this issue, see the following article: The Philosophical Problem with the Brain Disease Model of Addiction: Epiphenomenalism
How To End Addiction, Substance Dependence, Substance Abuse, Alcoholism, and General Drug and Alcohol Problems (updated 11/4/2015)
Due to the fact that most conventional rehab and addiction treatment programs follow the false belief that addiction is a disease, they are generally not effective at dealing with these problems – so I really can’t ethically recommend any “treatment” programs other than a run of the mill detoxification procedure if you feel you may be experiencing physical withdrawal symptoms – you can find that through your local hospital or emergency room; by asking your primary care doctor; or by calling 911 if you feel your life is in danger due to withdrawal (beware that withdrawal from alcohol and some prescription drugs such as the class known as benzodiazepines can lead to fatal seizures). But what comes after detoxification is simply personal choices, and treatment programs actually discourage productive personal choices by attempting to control people and feeding them nonsense such as the disease theory and idea of powerlessness.
If you want to end or alter your own substance use habits you need to make the choice to do so. Many readers will object to this answer as flippant, cruel, out of touch, et cetera. I realize this, but I chose to change, and in reality everyone who moves beyond problematic substance use chooses to change as well.
There is too much to unpack within what people believe is contained in the statement “choose to change.” I have tried to address some of that here in the past, but I realize this article is not the place to do that. This article’s scope needs to remain limited to the question of whether or not addiction is a disease.
My conclusion is that addiction is freely chosen behavior, and that the person who continues heavy substance use despite mounting costs still sees heavy substance use as their best viable option at the time they’re doing it – even though they recognize many costs and downsides. Choosing to change then, really means that they rethink whether heavy substance use is their best viable option. The only way I know to come to new conclusions is to re-examine the issues methodically, and this may often mean gathering new information and perspectives. Thus, the help that can be given to troubled heavy substance users is information. Helpers can provide accurate information that troubled people can use to change their perspective and come to believe they have better viable options than continued heavy problematic substance use.
I endeavor to give accurate information here that will help people to understand that change is possible, and that they are not doomed to a lifetime of addiction. Hopefully, this helps them on their way to believing in better viable options.
About this article:
I originally published this article on September 25, 2010. I have since added some significant supporting work I was able to find over the years, and those additions are noted. Some other minor edits from the original article are not noted.
Author
Hi, I’m, Steven Slate, the author of this post and of all content on this website. Yes, I was what you would call an “addict.” If you want to know more about me, go to the About page. If you want quotes from PhDs and such (as if I haven’t given enough here already) go to my Quotes From Experts About Addiction page. Please be civil in your comments, and many of your angry comments may already be answered on my FAQs page, so maybe check that out before you scream at me.
I agree that treatment facilities by and large don’t help. I’ve been to three over the years and kept “going back out there”. I even had a year sober about 9 years ago.
I believe that sobriety is a choice. I also believe that after years of rationalizing our addictions and covering up guilt with blame that we need some help to get back. No real change happened in my thinking until I wanted to be sober more than I wanted to be miserable. No treatment center in the world could have done that for me. That desire lead me to humility which lead me to ask for help which lead me to follow some suggestions from those who seemed to have what I wanted. I didn’t have to pay for any of that. Nothing at all was required of me. No one asked anything of me. No one devalued who I am, quite the opposite.
The only consistently respectful person in these comments has been the author of the article…Steven Slate. Believing that it is not a disease and AA harms society overall has no bad intentions attached. Everyone on both sides wants society to benefit. So calm down everyone and understand that. No one is a bad person here. There are a lot of rude people lol. I was really angry with papamick last time i was here…he really is a rude dude and doesnt see that it alienates the people he is trying to convince which is truly self defeating…but after a long break from here i realized he to has overall good intentions. He wants people to empower themselves. Nothing wrong with that. He could go about it in a nicer way, but that its his choice lol. I didnt like AA and it didnt help me, but I have to say that during the time I went i was never discouraged to have my own thoughts. I was told that that the program doesnt work for everyone, to take what i need and shove the rest, and was told about alternatives. It was not like a cult at all. Im an atheist and find more common religion like Christianity to be more cult like. Christians have told me I will go to hell if i dont think the way they do. Never heard anything near that harsh in Aa, but who knows mayber different places have different attitudes. I definetly left feeling brainwashed though. But tv is brainwashing, cable news shows like fox and cnn are brainwashing, so its kinda hard to avoid unless you are a hermit. I encourage people on both sides to really think about the other sides intentions before you start calling them evil or fucked or whatever. All i have seen here is good intentions. Everyone wants what is best for society, we just disagree what that is
But this is a very dangerous artical.
And trust me there are smart and not so smart people on both sides of this.
Oh and I dont think rehab and Aa create addicts. Drugs use creates addicts. I think an argument saying they keep people from getting better would be sound. I have met many people that it did work for. And btw those people in AA call themselves recovered and dont think of themselves as powerless. They think of themselves as powerless when they are actively using. Just to clear that up. They keep going to AA cause they feel it helps them stay sober and think helping others get clean is one way it helps. Some of them think they will use without the structure, some only think they will not be happy without it but wont use…what i am getting at is there are all kinds of people in there with varying thoughts. That was my experience at least
Fuck…i have to say one more thing about AA. I hope iy doesnt look like i am advocating it, cause i am not. I just had a lot of exposure to it. It needs to be said for clarity though. In AA and NA the title Addict is not the same as drug addict. They kinda made that up on their own. i took addict to mean someone who is profoundly more prone to addiction than the aberage person (addictive personality) , so when they say addict for life what they mean is you always have a strong potential to fall back into drug addiction compared to other people. It is kinda weird i must agree, they kinda made up the title addict. It is not something the science or medical community uses. So someone recovered in NA would still be an addict, but at the same time would be an ex drug addict. I personally just prefer to call myself ex drug addict and skip the addict title
As far as addiction being a choice i think it depends on the definition. Some defintions make it clear it is a choice while others make it clear it is not a choice.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3210595/#!po=10.5634
Yes, absolutely. And as far as sale of alcohol being a crime, it defends on the definition too. The current law in Afghanistan and Saudi Arabia, and the US from 1920 to 1933 define it as a crime, while most of the world’s countries now don’t.
The 12th century French law defined the Cathars and Waldensians as heretics, while there is currently no definition of heresy in France. The Malleus Maleficarum described and defined Satanic withches who were in league with the devil, and detailed the proper procedure to punish them.
Are there witches in the world? It all depends on the definition.
I don’t choose my biological reaction to alcohol. If I could choose to take one drink and not feel euphoric and lose control I would. I do CHOOSE to be sober. Sobriety is a choice. The rest of it is not.
And I want to be clear I think drug use is a choice but addiction might not be depending on the definition. Please read the entire contents of the link I posted in my previous comment for clarification. That means you too papamick lol
My new 12 steps:
1. We decided we were “Not Powerless” over alcohol/drugs – that our lives had become dominated by delusional 12 step egomaniacs.
2. Came to understand that we were never as morally reprehensible, intellectually challenged or spiritually deficient as some 12 step members had led us to believe.
3. Made a decision to turn and walk away from 12 step groups forever.
4. Made a scorching and fearless indictment against 12 step groups as organizations.
5. Admitted to Ourselves and another Human Being that We had been ambushed into joining a religious cult whose precepts are based on the juvenile occult theosophy of Frank Buchman and the new age spiritualism of the Oxford group.
6. Were entirely ready to relieve Ourselves of the self-defeating bullshit We were taught in the12 step dystopian world of delusion, [fake] brain disease, and “powerless” human misery.
7. Familiarized ourselves with cult indoctrination tactics in order that we [or our loved ones] may never fall into a similar trap again.
8. Made a list of all Occult 12 step disciples and acolytes who had harmed us, and became willing to confront them all.
9. Called such people on their bullshit whenever possible, except when to do so would significantly injure them or others.
10. Continued to indict 12 step groups and when we were wronged promptly expressed our disapproval of it.
11. Sought scientific empirical evidence that could help us to defeat addiction; focusing on ourselves as the Power to carry that out.
12. Having been awakened from the 12 step dystopian nightmare as a result of these steps, we tried to carry this message to other victims of these groups, so that everyone might know the truth about the failure of the 12 step ethos.
You twat!! Each to their own opinion. Not saying that yours is right. Don’t take the piss the 12 steps have saved lives. It’s a matter of life and deaf. Using against your own will is powerful enough. You need to know what your doing and what you are talking about!!!
The Occult 12 Step Ethos is particularly harmful to young people-especially teens. Sending kids to AA or other 12 Step programs- to the same rooms where judges are sending much older addicts and predators- is ABUSIVE. It’s also unconscionable to teach people in their teens that they have an incurable progressive lifelong disease over which they’re powerless.
In a nutshell, here is the 12 step dystopian model:
ALWAYS Hammering away at new comers and vulnerable young addicts with endless tales of human misery, oppression, and disease.
Years and years and years of browbeating, indoctrination and bullying–like: “you’re sick– you’re diseased– you’re insane– you’re best thinking got you here– you’ll never really recover– once and addict always an addict– you’re spiritually sick sick sick–you’re thinking is flawed– you have endless character defects that you’ll never be rid of– you can’t do it without US– your only alternative to a life of 12 step dystopia is “jails, institutions and death”— don’t think for yourself, it will kill you— Don’t use your logic- it will cause you to relapse– let your emotionally unbalanced sponsor do your thinking for you–without US your future only holds jails, institutions and death— Your “Intellect” and “pride” in self-empowerment will kill You— You are a victim, you were born with this disease and it’s getting worse-even if you stop using— You M U S T love and tolerate all reprehensible, criminal behavior otherwise you’re intolerant, unloving and hateful— you MUST accept US – this “group of drunks”- as your GOD– you MUST turn your life and will over to US because you can’t live life by yourself— you’re not a capable human being—– and on and on and on ad nauseam.
Going forward, let’s use a science based, logic based, reality based support system to help struggling addicts rather than the ineffective, diastrous 12 step ethos. Your C H O I CE —– 1935 Occult Spiritualism and Mindless Quackery or 2017 modern day science
Real help for addicts ***The Freedom Model *** As opposed to the current day Treatment center ***Control Model***
This is excellent from Baldwin Research:
“Why do addicts use drugs?” Treatment professionals answer: “Because they have a disease. Addicts can’t stop, no matter how badly they want to stop.” If this is true then human behavior is completely divorced from any sense of purpose; personal happiness isn’t a factor and people are seen as mere animals that need to be tamed and trained to do what’s good for them by those who know better.
When Control Model theorists see behaviors that they don’t approve of or are generally not accepted by society, they consider it to be evidence that the individual must be “out of control” and that they, the Control Model theorists, must step in to get them under control. If you shoot heroin or drink wine every night or smoke crack every weekend, you must need a professional’s help.
The professional recovery society is run by the Control Model theory. This unfortunate situation has been slowly coming to a boil through the inevitable and mounting belief that one group (the “professionals”) know what’s best for the other group (“the addicts, alcoholics, depressed, the anxiety ridden, mentally ill, etc.”)” –
See more at: http://www.baldwinresearch.com/the-freedom-model.cfm#sthash.4cUvrQhn.dpuf
Here’s one thing that has been on my mind for quite a while now: The research showing that there is a correlation between brain changes and self-reported desire.
The interesting thing is, when I decided to go to hospital for alcohol detox after having been a heavy drinker for years, I actually felt almost no desire at all during the stay there. And I felt very little desire for the next 3 months either, before some sad experience led to my decision to “self-medicate” again.
It would be interesting to know how valid that supposed correlation actually is.
Your choice friends——– The archaic1920’s Occult Spiritualism and Mindless Quackery of psycho Frank Buchman along with the preternatural 1930’s mystical magic of the Oxford Group — available to addicts in the 12 step dystopian model
….OR ….
21st Century Modern Medicine and the Modern Day Science of 2017
P.S. to the wet-behind-the-ears naive little puppy dog, Beau. 12 step organizations are NOT Christianity based- [sheesh, you’re such a numskull]
Once again. Why aren’t you able to do something other than rant and rave about how bad the 12 step programs suck? Instead of putting people down and telling them how stupid or how naive they are. Try helping someone ya dick! You are and egotistical, self centered asshole Papa Mickey mouse. You have off spring and as I said before hopefully your grand children do not become addicts on your watch. They will surely die a miserable death. Talk to your kids the way to speak to people here you condescending prick! Fuck off!
They called it the disease of addiction rather than the disease of diabetes or cancer because for eons, addiction was considered a character flaw and moral failing, that many still believe today, hence the emphasis by many on phrasing it as the “disease of addiction.” Like addiction, diabetes, cancer, or nearly any other “medical” disease will worsen or relapse if the person chooses not to take their medications, not to follow up with their treatment (whose methodology may vary for individuals), live an unhealthy lifestyle, eat the wrong foods, smoke, etc. I am sorry, the scientific community supports genetic predisposition, physiologic changes which affect usage, and environmental/poor coping skills (which again will affect ANY disease) as causal in addiction. The percent attributed to each of those factors may be different in individual persons, some more a factor than others, just like many other diseases. That may not suit what others want to sell, but maybe we could defocus on selling and get about helping each other using whatever methodology works. We are only recently finding meds that help addiction. Many diseases, including mental illness, epilepsy, cancers, etc require trialing a variety of medications for different individuals before results can be obtained. A med that works for one person with the same disease, will not work for another person. It is a complex mechanism, and drugs and other treatments will continue to evolve. Addiction is a multi-treatment modality just like any other disease (in orthopedics, it might be medication + physical therapy + lifestyle changes, etc). Maybe less arguing about it and more multiple approach treatments.
Why do people have such a need to argue? There’s no point. Most of the time people are going to believe what they already believe based on their own limited biased experience. I know what I know about myself and others based on what I’ve experienced. I have a lot of “issues”. Anyone who tries to tell me that I don’t have what I have has simply never walked a day in my shoes. They’ll never really know what it’s like. And that’s ok. I’m glad they don’t know what it’s like because it’s not something I’d wish upon anyone really. Good for them. They don’t suffer like I do. I’m not going to try to make them understand when they don’t have the capacity to know what true darkness is. I know there are many others like me. I don’t need to suffer alone in silence. This website is entertaining at best. At worst it’s just another guy using a platform to twist studies around into ways that agrees with how he can understand addiction. Maybe this is how he really needs to believe it to be for himself. Maybe that is how he stays sober. Good for him. To each his own. Live and let live. Life is hard enough. I just know what works for me. I am grateful for the field of recovery. Without “moments of clarity”, and knowing where and how to get help, I wouldn’t be here anymore.
Most of these “In-Patient Rehabs” are out of network operations setup purely to make as much money as possible. They acheive this from super high daily rates touting 100% cure rates and making tons of money from uneccesary drug testing. ( although insurance companies are craking down on this) I would consider these businesses to be in the travel industry not the rehab medical profession. They all locate themselves in sunny beach locations and offer all types of amenties that you would find at a 5 star hotel/resort. None of this will actually help you cure any addiction especially an opiate addiction. If you look at “In-Network Medicaid” facilities the average cost is usally around $200/day or $6k per month!!! They might not be located next to the beach but they offer the same treatment really in a less beautiful setting! I personally dont care how pretty the scene is and dont think it would matter one bite when I am withdrawing from Heroin or Oxycodone!!!! The last thing you are going to want to do is get a message or run on the beach ridding horses!! If you have been through opiate withdrawal you know exactly what I mean. So its my opinion that if you are going to go the route of In-patient treatment just find the best local facility that your insurance will cover ( most people are on medicaid once they reach this point or non at all ) and save your family tens of thousands of dollars for a 3-4% chance that you will stay clean after that 30 day stay. You could always try MAT ( Buprenorphine or Methadone ) for $3,000- $5,000 per year which works out to around $11/day and has a much higher success rate for opiate addiciton
The description of addict as a disease is, in part, is a service to those with an addiction. Obviously, one of the factors that keeps victims from embracing sobriety is guilt. “I eat because I’m in happy, and I’m in happy because I eat” – fat bastard. Every time your high you say “this is it, I hate this, never again,” and in that moment you mean what you say with all of your being. Once it wears off, your first thought is you need it. One reason may be physical dependency, however the other is guilt. In many cases, you have to do things that’s are less than honorable to maintain the addiction. For example, stealing and selling your dead grandmother jewelry and watching your mom cry when she finds out.
Describing addiction as a disease is like say “it’s not your fault.” Now addicts have a way to live with themselves once they are clean. Now detox is a little less scary/ acceptable. They are being treated for their disease.
Everyone who has billed insurance for either subutex, suboxone, methadone, or addiction counseling, knows that these are covered under the title of “behavioral health.” Who treats addicts? Psychiatrists. Radiologists and pathologists aren’t involved. The desire to provide diagnostic images as a means of proof, is because this is what is used to diagnose or rule out pathology (some times in conjunction with a biopsy). Addiction is the psychological disorder in which there is an individual who cannot properly cope with emotions. Some think it makes them cool(low self confidence), some are introduced by another user and are drawn to the euphoria, form an addiction and subsequent guilt, some have a lack of positively affirming activities which make them feel useful, productive, or needed, and for many it’s boredom. Any you know you have hit the pantry when bored.
As far as NA you have to keep in mind that there are those who have chosen to be there an those who are court/parent appointed. You mix the sincere with those who are counting down the days when they don’t have to be there anymore. Then one day as everyone is murdering coffee and cigarettes they are standing next to someone who’s high right there and and says to the guy with aches, sweats, and chills “I got if you need.” Sure it’s a choice but its like asking someone “I can make your severe flu symptoms go away instantly, interested?” The key is changing people places and things, perhaps with a substitute drug so your not too afraid to make the first step, and removing the “choice all together.” The only reason I would say that it’s a disease is because after detox until death you will be controlled by it one way or another. Fighting to get it or fighting to stay away. Like they say “once a druggy, always a druggy”
It is funny that you do not define substance use as a compulsion but washing your hands to the point your skin falls off is a compulsion.
That does not make sense.
Disease definition – a disorder of structure or function in a human, animal, or plant, especially one that produces specific signs or symptoms or that affects a specific location and is not simply a direct result of physical injury.
or
a particular quality, habit, or disposition regarded as adversely affecting a person or group of people.
Addiction surely sounds very disease like.
I think it is awesome that you considered yourself what we would call an addict but made the wonderful noble choice of sobriety! Congratulations! To not -be an addict is really not the desire for those of us who, well, have decided not to make the choice to be and stay clean and sober. Millions upon millions of us would rather loose our jobs, our families, our friends, our homes, our freedom and our lives. We choose not to have those things because those things just do not matter to us. We choose what really matters, and that is to be addicted to drugs. Because needing to be high has so many rewards and is so much better than anything else we have ever experienced!
I wish I was you! You are magnificent!
If I choose to be you, than I could, be you, right?
In less than 2 days, 3 people that I know have committed suicide because they became so tormented by their “choice” to be addicted to drugs.
They didn’t choose addiction any more than you chose not to be addicted! They chose death to make it stop! Your not helping anyone with this blog. Or is that what you choose to do with your information. Not help!
I was just on the back end of this site approving comments, and so many of the comments left on this page are all about Alcoholics Anonymous/12 Step programs. I sit there asking myself – “is this article about AA???” The answer of course is that it’s not, and to make sure, I searched this page for all sorts of keywords that mention these programs specifically. Of course, it comes up countless times in the comments – but in my actual article? It only comes up TWICE in this 7045 word article.
Again – there are seven thousand and forty five words in this article. Among those 7045 words, “12 step” comes up exactly twice. One instance was in a sentence pondering the likely “treatment” received by Nora Volkow’s meth-addict brain scan subjects, and it reads:
That can’t be read as an AA criticism in any possible way.
The next instance is offhandedly critical:
That’s it for mentions of 12 step programs in this 7045 word article. I hardly see how that warrants a non-stop argument about AA in the comments here. Please, for the love of god – bring the AA argument somewhere else. This article is about the brain disease model of addiction.
-Steven Slate
This, what you’re doing right now, is fucking irresponsible. You can’t observe a drug producing mainly psychological adiction (i.e. Meth) and apply the observations to all addicts. Have you ever seen an alcoholic or opioid addict or benzodiazepine or barbiturate addict in withdrawal? If they don’t have it in their system, they get violently ill. Withdrawal from barbiturates, benzos, and alcohol can actually kill someone. Now look me in the fucking eye and tell me they have a choice to use or not. Dont think about usinf the “if they hadnt tried it in the first place” argument; most addictions start with a doctor’s prescripton or mental illness; and if the patient has the addiction gene they’re pretty much up shit creek. Diabetics get very sick if they dont have insulin, would you tell them insulin is a choice? Where I live, we have peple dropping like flies and a fentanyl epidemic. We have very effective medical treatment options, but the wait lists are 3 months minimum. If we funded it more, we could treat far more addicts, and the fentanyl would disappear with the market for it. It would even save public health funds by reducing the number of OD’d addicts in the ER. Governments don’t want to fund it because of bullshit opinions like yours (and AA/NA) that condemn addicts as “less than” or “all violent criminals). Until that changes, people will keep dying. So fuck you, I hope you enjoy the blood on your hands. Waste of fucking air.
Hi JD,
You said “You can’t observe a drug producing mainly psychological adiction (i.e. Meth) and apply the observations to all addicts.”
So, I’ll expect you to head over to NIDA and voice this criticism to them, because they are the ones who repeatedly use the brain scans of meth users to justify their brain disease theory and apply it “to all addicts.” Here’s one prominent place where they do that: https://www.drugabuse.gov/sites/default/files/soa_2014.pdf
You see, I can only analyze the claims in the form they put forward, and that’s how they’ve presented the brain disease model specifically – which is what this article is about, specifically.
Regarding the issue of withdrawal – it is a side issue to the notion of “addiction”, as NIDA says in answer to the question “Is there a difference between physical dependence and addiction?”
Only a tiny percentage of people considered to be addicted have the kind of life threatening withdrawal symptoms you raise here. If they need help with that, it is available at most local hospitals. At the bottom of this, and every page on this website there is a brief mention of the issue of withdrawal, as well as a link to SAMHSA’s treatment locator for readers to find detoxification help if they feel they need it. Opiate withdrawal is almost never life threatening, except in extremely rare cases where other health problems present complications. I was a heavy IV heroin user, and went through withdrawal countless times without detox treatment – that is, I CHOSE to go through sickness rather than to use more heroin. I am not alone in this, nor am I a super human of any kind – most opiate users have gone through withdrawal unassisted. That is, opiate withdrawal doesn’t compel people to use. Nor, for that matter does withdrawal from other drugs – it forces people to be sick, not to continually use massive amounts of substances. It was a common practice in hospitals at one time, to aid in alcohol detoxification by giving alcohol users decreasing doses of alcohol. Of course, anyone could do this themselves, but they often don’t, because they want the effects of alcohol or whatever other drug they’re taking. And of course in the vast majority of cases, those alcohol users are free to leave the detox clinic at any given moment and resume heavy drinking. When they stay to fully detoxify, they do so of their own free will – i.e. BY CHOICE.
You won’t find me making the: “if they hadnt tried it in the first place” argument. In fact, I’ve argued against that on my FAQs page.
Withdrawal isn’t the issue, it’s a side issue that results when quitting. It is it’s own medical issue. The fact that so many people become fully detoxified and then begin using substances at levels/frequencies that develop physical dependence all over again is a testament to this fact.
Open and read this link and it will tell you that it is a chronic disease.
https://medlineplus.gov/magazine/issues/spring07/articles/spring07pg14-17.html
Did you read this article before you started commenting? I used the presentation in “Drugs Brains, and Behavior” (the booklet put out by NIDA and referenced in the link you posted) as the standard presentation of the brain disease model against which I’m arguing on this very page. I reference it within the first few paragraphs of the article, and quote and refer to it quite a few times throughout. That is to say, telling me to read it because “it will tell you that it is a chronic disease” isn’t a counterargument on your part whatsoever. It’s a mere appeal to authority – and specifically, an appeal to an authority whose claims I’ve already argued against extensively here, and cited several experts (including an accomplished neuroscientist) in support of my arguments.
It’s a shame really that the comments section has gone completely spaz and off the point. Now nobody seems to be talking about ‘Brain Disease’ and are mud-slinging ‘My Dad’s bigger than your Dad’ crap. My method works, your method doesn’t and is killing people. I find this always seems to happen in circles where addiction is discussed. It’s tribal nonsense. We have people coming in to comment who clearly have not read the article, adamant that they not only know what the article is about, but that they will damn sure stick up for the method of recovery they have chosen. It’s all just gross assumptions on a large scale. I’m out. I hope you all find piece in whatever method you choose, but above all that it is successful.
Fantastic article, thank you.
You mentioned, very briefly, depression.
“The phenomenon of brain changes isn’t isolated to “addicts” or anyone else with a so-called brain disease – non-addicted and non-depressed and non-[insert brain disease of the week here] people experience neural adaptations too.”
I am curious, is there a similar way of thinking regarding depression?
From The Emperor’s New Drugs, by Irving Kirsch:
I LOVE THIS ARTICLE!!! 100% AS SOMEONE WHO WAS ADDICTED TO HEROIN AND COCAINE FOR 37 YEARS, I KNOW THIS IS TRUE.
Convincing people that they are lifelong “addicts” without free will is the best way to prevent their recovery.
[That means-don’t brainwash people into believing they have a chronic progressive brain disease & don’t bulldoze & bully them into a fictitious belief in a powerless existence]
An important study led by University of New Mexico psychologist William Miller found that two critical factors predicted relapse for those treated for alcohol problems: “lack of coping skills and belief in the disease model of alcoholism.”
University of New Mexico = http://bit.ly/2dhSLD7
[Fake] Brain Disease 12 step programs insist that you maintain your alcohol and/or drug focused life so that you can continue drinking or drugging while pleading that you are “powerless” over your “disease.” Those who can kick the [fake] brain disease 12 step habit, are those who have something other than alcohol and/or drugs to build their lives around.
I’ve seen changes in people who work the 12 steps. People who have nothing now have something. The way you are slating the 12 is discussing as it could save lives. It’s all about choice what works for an individual. Your message comes across very toxic against AA. Be careful and be mindful if any addict comes across what you’ve written because you give them the feeling of no hope and scare them away from something that can save their life, could end dead with the influence of your words.
Ozi
Stop with the fear-based B.S.
Stop your bullying. Look, if it doesn’t work for YOU, fine. That doesn’t mean it doesn’t work for anybody else. To think that, is to be based in egocentrism, EGO (part of the addict’s problem). I worked in a 12-step treatment program. I have friends and relatives who work a 12-step program with YEARS of sobriety. If it works for ONE person, it is a valid method. Too scared, skeptical, and/or spiritually underdeveloped/proud for a 12-step, fine, pick another method. There is no one magic bullet, no shot you can take for it. Whatever flips your switch and gets results.
In the real world, DARLENE, we base success on that which can be tested, peer reviewed, and proven. Sadly 12 step programs are snake oil. If religion, spirituality, or neo-spirituality rooted in Oxford Group juvenile fairytales and the psychotic rantings of an unsuccessful stock trader could cure mental health issues it would be tantamount to aliens making first contact.
You have no idea how the brain works and you are only hurting addicts and their aid for help. Please. Stop and do something you actually know about. R u an addict? Do u have a child with addiction? Have you lose someone to addiction. Please learn the brain and mental behavior PLEASE
I Truly enjoyed all the information here. Thank you Steven…and you are funny too. Im not posting to agree or disagree. Im not a Medical doc Scientist Psyciatrist etc…I am recovered although from Drugs (Meth cocaine opiates shooting smoking snorting.) And Alcoholic (Whisky) for approximately 45 years. I like the idea that WeAreAll Just trying to Help by what ever means possible (yours..information) So All I really want to say is this… After such prolonged Negative Behaviour Repeated Over & Over it can be Extremely Difficult or maybe even impossible in some cases to SEE another path Alternate Route CHOICE as you called it…. Now here is my Point….CHOICE IS DONE IN THE MIND…following through requires ACTION a Motion Physical Movement….HERE STEVEN is where we might need Outside help because my Brain forgot the pattern to follow the positive Route..Show me and I will Copy you. I agree with you I believe you I also know that AA at one time…Saved my Life…taught me some really good patterns to follow. I’m no longer a AA attendee BUT I applaud them for their efforts Love of Humanity and Vision of a Healthier Life….I do Not DO NOT agree w/some of their Teachings But that by no means Discredits the whole program or does it make them Wrong or Bad. Many Many lives are saved salvaged and go on to be Happy Humanitarians. I personally used it as a learning tool a stepping stone I picked up a lot of GREAT habits from AA and left the rest. At some point my Mind and Soul the Heart of who I am as a Human Being yearned for more…Growing requires Change so for me AA was a great piece of cake…But I want the whole Cake. Im no Longer a PRACTICING Drug addict or Alcoholic BUT STEVEN someone had to Physically SHOW ME ANOTHER PATTERN TO FOLLOW FIRST….before I could CHOSE in my mind an Alternate Route. Then with the help of other human beings I followed through with Action. Thank you for your time and Attention. Cathy K. ✌
To be plain, there is ample evidence that AA is in reality a religious cult masquerading as a self-help group. Its adherents actively indoctrinate newcomers to their way of thinking using overt and subtle misinformation, intimidation, and false promises. They routinely prey on a population subset of sick people at their weakest, namely desperate alcoholics. Through ancillary groups like Al-Anon and Alateen, AA also attempts tobring the families of alcoholics into their cult. Unless AA offers something tangible, verifiable, and repeatedly helpful to these people, it is not just deceitful but dangerous.
In my Experience of different AA groups Sir…different States…different towns…different years Never Ever was intimadation used And Of course its directed at Sick and Suffering and Desperate because that is WHO the program is for. I agree that there is some Misinformation tho….But there is where my Agreement with you stops. If you look at the number of lives it has changed SAVED and brought New purpose into the Minds of Human Beings so that Now they are Useful Compassionate Healthy Contributing Free Spirited people to any community…Something is Good and Right about that program that you are FREE TO JOIN OR FREE TO LEAVE AT ANY TIME. And furthermore the Promises were Not false at All it fulfilled each one for me and countless others that I personally know. But Again I am Not Now a AA member because As THEY SAY Very Clearly TAKE WHAT YOU NEED AND LEAVE THE REST! And I Did. So infact where I was POWERLESS (Over my situation) Now I am Not. PEACE ✌
Cathy wrote: “AA and the truth .. has worked for millions upon Millions….”
We often hear this from brainwashed 12 step acolytes. It’s pure nonsense. It’s interesting how Cathy links AA and Truth. LOL. The ‘truth’ definitely helps addicts to recover. 12 step programs rarely do. The truth is that the available evidence strongly suggests that 12 step treatment provides very little or no long-term help for active addicts/alcoholics. Further, there is ample evidence that long-term repeated exposure to these programs is actually dangerous to many addicts/alcoholics who would fare better if left on their own.
There is ZERO scientific evidence that suggests 12 step programs have helped ‘MILLIONS’ of addicts to recover. No published statistics and no studies to corroborate this childish MYTH. But there is a plethora of published scientific evidence in the form of statistics and studies that proves the opposite. 12 step programs do more harm than good. Dystopian 12 step programs are Faith-Based, Not Evidence-Based.
Neither A.A./N.A. etc nor many other SATs [Substance Abuse Treatments] are based on science, nor do they seem interested in doing any scientific studies which might test whether the treatment they give is effective.
Surely we can do better than juvenile 12 step programs. If three-quarters of alcoholics/addicts can stop drinking/drugging on their own with no treatment, we should be looking for ways to help them succeed rather than imposing a treatment that has not been proven effective and that may actually make things worse.
Steven I just wanted to clarify that my comments on AA were not directed at you BUT directed at the Negative Bashers in the Comments who completly Destroy AA and the truth might be It Did Not Work for YOU BUT has worked for millions upon Millions….and why does it work? Because it teaches ALTERNATE HEALTHY BEHAVIOR MODIFICATION. IF infact it were a Hopeless state of Mind & Body as they Claim Behavior Modification would not work right? For u synics “It works IF U….AGAIN U WORK IT” how do you do that? Chose then follow through with Action. Again I AM NOT A AA MEMBER ANYMORE
Sorry for the rant…Again Thank u for the info. I agree to agree. 💜✌
Recovering alcoholics are taught by AA to give all credit to God and AA. They generally oblige, regardless of any other external or internal factors that tend to keep them sober, such as an honest desire to be healthy again or the love and support of their families. AA denies these influences, and The Big Book even admonishes AA devotees to put family third after God and AA and to put everything else in life last.
Why would anyone want to constantly focus on the misery of a dreary and blighted drug addled past? Why would anyone want to spend so much time confessing [sharing] character defects, personality flaws, failures and mistakes and then pretend that they are ‘Portals’ to discovery that lead to spiritual progress?
It’s very odd to do that. It’s dystopian in nature. For me, the portals of discovery are reality, truth, reason, logic, success, soundness and virtue. The 12 step promise that states, “We will not regret the past nor wish to shut the door on it” is counterproductive-even harmful. Why? Why would anyone want to always [on a daily basis] relive the desolate and bleak experiences of a fractured and dismal past? It’s senseless and shameful.
It doesn’t help anyone.
I look not to the past but rather to the future because that’s where I’m going to spend the rest of my life. The future belongs to those who believe in the beauty of their dreams.
Many addicts use to cover, suppress and obliterate their feelings, their fears, their sadness, their guilt, their shame, their inferiority (essentially the ego). They may deny their weaknesses, exaggerate their strengths, or vice versa. They may have distorted insight into their problems, and their abilities. Their insight, judgment, reasoning and thinking may have become impaired with chemicals There is an expression in 12-steps (and beyond), that each day is a new beginning. Every day, we still have failures, weaknesses, fears, etc. That never ends. That is why a person needs to be in touch with them, know them, understand them, admit/acknowledge them, have the ability to address them…every day. “Confession” can be good for the soul, whether it is journaling or speaking them in a group (for some just hearing them from others) and can be powerfully helpful. My addicted relative in his early sobriety would say, each minute is a new beginning, and he would literally go down on his knees in prayer and attend several AA meetings in a day to stay sober. He has been sober for 40 years, and he believes it is the ONLY way to achieve sobriety…though again, we are all unique individuals with different chemical compositions and functioning, with different levels of development and receptivity. Choose what gets the desired result.
Sorry Papamick But if YOU reread my post you will see that I did not link AA AND THE TRUTH what I said and forgot the Comma was that The truth might be it did not work for you. Please do not quote me Unless you can do it correctly. I also Very Clearly stated (you might want to reread it if you are going to quote it and rip it apart w/your Negative Nonsence) that I do not agree reread that I do not agree with all there claims one being..”.Hopeless State ” for that clearly is NOT True or Behavior Modification would not work. Second being “I am no Longer a Member” why?? Because I learned a few Very Useful things New Patterns of Living and Guess What THEY LET ME LEAVE ha ha…no one tried to stop me at the door forcefully in any way whatsoever I left Freely with MUCH MORE then I arrived with. Brainwashed….yes Sir and Boy did my Drug infested and Alcohol soaked Brain need washing. Peace Sir you might want to direct your Negativity and Anger or what ever that is Dripping from your sarcastic words at something that is actually hurting or destroying lives Not at something that is making them Better just because you disagree. ✌
Instead of telling people they are powerless, wouldn’t it make more sense to empower them and build on their strengths? Why not tell them they are stronger than alcohol and they can choose not to let it control them? Even if you prefer a religious approach, you could pray for God to support your strength to change your own life, taking full personal responsibility rather than passively turning over the responsibility to a higher power. The old adage “God helps those who help themselves” applies.
Instead of the religious model of sin, confession and absolution, what if we avoided harping on the past and started fresh, concentrating on the patient’s behavior today and in the future? Sure, make amends to those you have harmed for the bad things you have done, but why not put the emphasis on doing good things for other people today and tomorrow? Instead of being “ready to let God remove your shortcomings,” how about taking active steps to improve your own behavior? Why not build self-esteem instead of re-visiting past experiences that damaged self-esteem?
Actually empowering them is exactly what they do…restoring self-esteem….they do that too and Many other good SUGGESTIONS they do that too! Im beginning to realize YOU actually know NOTHING about Their program!! Good day oh and PEACE.