There are a lot of issues involved with determining success rates for the various programs designed to help people with substance use problems. But how is success measured, that is, what constitutes success? Is it the reduction of substance use itself? Is it abstinence? Or is it the reduction of substance use related problems (less arrests, and/or better functioning in work and social situations)? Everyone seems to have different criteria for this. I think the most absurd criteria for success is whether or not people stay in and comply with treatment programs (retention). Witness this recent example of retention rates being conflated with success rates:
Mid Coast Hospital’s Addiction Resource Center has received national recognition from the Network for the Improvement of Addiction Treatment (NIATx) for increasing access to science-based treatment protocols for addiction toprescription opioid drugs such as Codeine, Morphine, Oxycodone, Hydrocodone, and Fentanyl; and illicit drugs such as heroin.
Opening the door to such treatment in the Mid Coast region has resulted in improved patient access and outcomes. Wait times for treatment were reduced from 11 days to 2.5 days from first call for help, engagement (staying in treatment) improved from 20% to 85%, and treatment completion rates improved from 60% to 94%.
Highlighting the success of this approach to addiction treatment, Haram continued, “Through this process we were able to provide treatment to 200 more people per year, without any new state or federal dollars. In addition to this, the increased volumes brought the actual cost of treatment down 30% per person.”
This is from the hospital’s website. Here’s a newspaper article where they cry about potential cuts to this “successful” program (those quotes are meant as sarcasm, in case you couldn’t tell).
They mention improved patient outcomes – where are the statistics on that? No answer is given. One would think that if they had evidence of improved patient outcomes then they’d certainly offer it up. Instead, they give us irrelevant statistics. This treatment center was declared a success, but the fact that they were able to get more people into the program and keep them there longer says nothing about whether the treatment is successful or not. Retention, engagement, and completion rates are for the most part, nonsense. If you have a program that works, then it’s good to have high retention rates, and that means you’ll help more people. But they skip right over measuring whether the program actually works, and declare retention rates as evidence of success. It may be a success for the bookkeepers, but I’m afraid the people being treated probably aren’t that much better off.
Such distortions are not isolated to this example, they’re part of a horrible trend in the treatment industry, which has basically given up on trying to objectively measure whether their programs actually help anyone, and instead simply measure whether people stay in the program, how long they stay in it, or whether one particular ineffective program is more “cost-effective” than another ineffective program. Since none of them actually beat the known rates of natural recovery, then none of them are really “cost effective”. They’re all a waste.
What you’ll find out if you really start looking into treatment programs for addiction is that almost none of them are able to tell you what percentage of people actually stay sober after leaving the program (“patient outcomes” as mentioned above). Having given up on trying to objectively prove that their programs work, most treatment centers now say that “relapse is a part of recovery”, declare that addiction is an incurable disease, and compare it to diabetes or asthma as a means to excuse their own failures in getting through to people – as exemplified by this statement from the NIDA:
A Deceptive Comparison by the NIDA
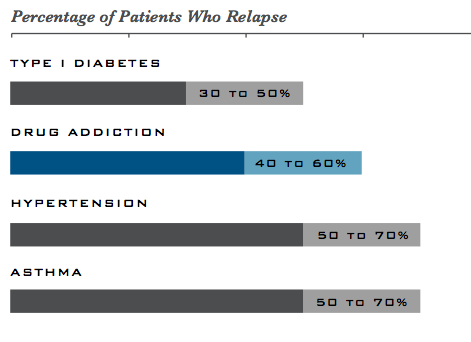
The chronic nature of the disease means that relapsing to drug abuse is not only possible but also likely, with relapse rates similar to those for other well-characterized chronic medical illnesses—such as diabetes, hypertension, and asthma (see figure, “Comparison of Relapse Rates Between Drug Addiction and Other Chronic Illnesses”)—that also have both physiological and behavioral components.
Unfortunately, when relapse occurs many deem treatment a failure. This is not the case: successful treatment for addiction typically requires continual evaluation and modification as appropriate, similar to the approach taken for other chronic diseases. For example, when a patient is receiving active treatment for hypertension and symptoms decrease, treatment is deemed successful, even though symptoms may recur when treatment is discontinued. For the addicted patient, lapses to drug abuse do not indicate failure—rather, they signify that treatment needs to be reinstated or adjusted, or that alternate treatment is needed
With such leadership from our government, it’s no wonder that these treatment centers feel no need to show long-term success. Achieving a true success – which I would define as a person leaving their addiction in the past and moving on with life – has been officially deemed impossible. Success has been redefined, and is instead measured by a program’s ability to keep someone in treatment for life. This totally gels with the recovery culture’s claim that you can never become “recovered” and that you can only be in a constant state of “recovery” which of course includes a “one day at a time” lifelong struggle with addiction and repeated cycles through treatment programs. The treatment centers call this “managing your disease.” Witness this nonsense from an upscale inpatient program:
For a long time alcohol treatment success was measured by whether or not the individual relapsed once the program was complete. This method is misleading in some ways. Experts have found that alcoholism is a disease like any other – and the individual who goes into “remission” or a recovery stage may indeed relapse over the course of their life. Thinking about alcoholism in these terms, it is hard to judge a program based only on relapse rates. Instead, programs must be judged successful in terms of how well they help their patients manage their disease.
Ah yes, the disease – what started out as a misguided understanding of substance use problems has now become the perfect marketing tool. More wisdom from the NIDA:
Treatment dropout is one of the major problems encountered by treatment programs; therefore, motivational techniques that can keep patients engaged will also improve outcomes. By viewing addiction as a chronic disease and offering continuing care and monitoring, programs can succeed, but this will often require multiple episodes of treatment and readily readmitting patients that have relapsed.
“By viewing addiction as a chronic disease” you can essentially throw all of your money down the drain on a life of treatment, and waste your life away, being brainwashed each time to believe that your disease will strike again and that “relapse” is inevitable. Treatment programs are just telling people to spend more and more time in treatment, as a 2008 report from Join Together proudly shows:
The Betty Ford Center in Rancho Mirage, Calif., for example, now has a 90-day residential treatment program. More than 50 percent of the clients in Promises Treatment Center in Malibu are in 45- to 90-day treatment programs; the young-adult program at Promises has been extended from 30 days to 90 days.
Visions, an adolescent addiction center in Malibu, increased its program length from 30 days to 45. Hazelden also is expanding to meet the demands for treatment programs of 90 days or more.
Although 28- or 30-day treatment programs are still common, addiction experts say that longer treatment programs will help to curtail the cycle of hospitalization and relapse.
“There was a belief that 30 days was the right number,” said David Sack, chief executive of Promises and an addiction psychiatrist. “But there was absolutely no data to say 30 days was the right number. What we’re seeing now is this much broader view for how to manage addiction.”
To what end? Does it actually create success. According to that report, longer stays can double the success rate of treatment – from 17 to 35% – this is still horrifically low (not to mention they don’t cite the exact source for those numbers, so I don’t know how reliable they are) – the fact that they would brag about such numbers is appalling. On the comments of the above article, an employee of a California rehab states:
Our experience in 4-6 month residential treatment is that 30-35% of admissions get clean and are still clean and sober at the 6-month follow up — a great outcome that makes a good case for long-term treatment.
It doesn’t make a great case for long-term treatment! At any given moment, 75% of people who could be diagnosed as ever having “alcohol dependence” in their life, and who haven’t been to a treatment program – are currently free of alcohol dependence. Most people get over their substance use problems whether or not they get any “treatment.” If you wanna impress me, show me that people are actually better off in the long run having gone through your program, that is, show me that you’re helping people who wouldn’t have “recovered” on their own, or show me that you help people to change quicker than they would on their own – but don’t brag about a 30-35% success rate, because that’s just pathetic. It gets worse too. Many programs are now advising people to spend a year or more in treatment, and I recently heard from someone who sent their child to an 18-month program at the tune of $80,000! Imagine the wonders you could teach your child with that much money. You could send them on a trip around the world for a year and a half, get them into college, or help them to start a business and experience real fulfilling success in a productive lifestyle – any of these experiences would be a far better option than wasting your time at a treatment center, sequestered from and learning nothing about life in the real world.
Many in the treatment world are beginning to understand just how pathetic their real success rates would actually sound. This is why they’ve turned instead to talking about retention rates and whatnot. Saying “treatment completion rates improved from 60% to 94%” sounds far better than saying that you have a 35% success rate – but it doesn’t change the fact that your program is a failure. Ultimately, everyone who successfully ends their substance use problem chooses to end it, chooses to change their behavior, and chooses to move on with their life. Accordingly the goal in helping people should essentially be to persuade them to make these choices, and help them to develop the tools to do so (the tools lie in understanding the processes of decision-making, and in implementing an alternative more satisfying lifestyle than that of addiction). This however is not the goal of treatment programs. Their goal is only to persuade you to believe that you have a disease which robs of the ability to make your own choices, and that you’ll need treatment for the rest of your life. Unfortunately for people who want real help, they’re getting better and better at achieving this goal.
By Steven Slate
Steven Slate has personally taught hundreds of people how to change their substance use habits through choice - while avoiding the harmful recovery culture and disease model of addiction.
What a terrific article!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
The good news is that this is all about to change. twelve-step and rehab will be a thing of the past in the next 5 to 10 years with the introduction of truly effective treatments based on our new understanding of addiction as a disease of impaired neuroplasticity. The discovery of the glutamate receptor in extinction learning and drugs in development that exploit this (d-cycloserine, etc.) will make all of this seem primitive.
As an addict, I agree with the comment above that addiction will ultimately be solved with medication rather than 12 step programs.

What a terrific article!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
The good news is that this is all about to change. twelve-step and rehab will be a thing of the past in the next 5 to 10 years with the introduction of truly effective treatments based on our new understanding of addiction as a disease of impaired neuroplasticity. The discovery of the glutamate receptor in extinction learning and drugs in development that exploit this (d-cycloserine, etc.) will make all of this seem primitive.
As an addict, I agree with the comment above that addiction will ultimately be solved with medication rather than 12 step programs.