I get many communications from rehabs and recovery organizations trying to get me to post an infographic full of addiction myths, or to advertise a rehab on my site that I completely disagree with, to propagate some content I disagree with, or to vaguely work together in some way.
One of the recent messages I received was from a fully disease-based chain of rehabs/treatment centers that sets people up in long-term treatment plan with outpatient following inpatient. They wished to somehow work together to end shame & stigma. They thought I and my website could somehow be involved with them. It’s not uncommon that they like so many others, seemed to have no idea what I believe here, while asking me to help promote their ideas. Here is my response:
Response to unnamed treatment center chain:
Hi Carli,
I think we see things very differently.
Regarding Stigma. I don’t believe that the disease model of addiction reduces stigma: see this blog post reviewing some research:
http://www.thecleanslate.org/the-never-ending-stigma-battle/
“The study compares survey data for 1996 and 2006, over this time period public acceptance of addiction as a neurobiological condition increased 9 points, the number of people who see it as a chemical imbalance also rose by 9 percentage points, and the number of people who see addiction as genetically caused rose by 10 points. The same study shows that the number of people who would be comfortable with an addict as a neighbor went down by 5 points, that less people would want to socialize with an addict, and the other stigma measures remained relatively unchanged compared to the great gains in acceptance of the disease view of addiction. Essentially more and more people are coming to accept addiction as a disease, but this isn’t putting a dent in the stigma, which is getting worse in some ways.”
Regarding Shame: I think the disease model works to create more, and that a free choice model of addiction does not have to include shame, see this blog post:
http://www.thecleanslate.org/choice-isnt-shame-shame-choice/
“We all know that shame and guilt are related to behaviors perceived as negative, but I don’t think most people realize the defining feature of shame: “I am bad.” That little bit of self-talk is what would be called in theories of attribution, a “stable” attribution – which means that the person thinks of the cause of the behavior as a permanent unchangeable condition. “I AM BAD” doesn’t allow for a different choice, it doesn’t allow for a mistake or misjudgment, and thus it doesn’t allow for better outcomes in future similar situations – it means that you are fundamentally flawed – that your very nature will always lead to such behaviors/outcomes.
Viewing yourself as having fixed psychological/behavioral “traits”, abilities, or “talents” is also a matter of stable attributions – or as another prolific researcher, Carol Dweck calls it, a “fixed mindset.” It’s a way of thought that can be damaging even when applied to positive attributes. For example, someone who thinks that they are intelligent but that their level of intelligence was born into them as a stable unchanging trait will tend to fall apart when faced with challenges and then limit their efforts so that they avoid any potential challenges – because they view difficulties and the need for effort as a sign that they’ve reached the limits of their intelligence.
So for shame to set in, the individual must first judge their behavior as bad, and then they must internalize that badness – thinking of it as a stable unchanging part of their very basic nature or identity.
Contrary to the unending claims that believing addiction to be caused by an incurable disease would absolve people of shame, it actually PROMOTES this sort of thinking. In the disease model of addiction you are taught to think of yourself as having an incurable disease; a fatal flaw; a trait that will forever be with you.”
Regarding unending engagement in treatment or support for recovery – there is no evidence that longer treatment is better, none. There is some correlation that people who continue to go to meetings have a higher rate of success, but this is a self-selecting group – that is those people are committed to change, therefore they go to meetings because it’s what they’re told to, but they’d be fine without the meetings to. Those who drop out quicker are less committed. In short, meeting attendance or even treatment attendance doesn’t cause recovery – it’s the other way around, a strong commitment to recovery causes meeting and treatment attendance.
See this article on Project MATCH data, a $35 Million study carried out by the US government on outpatient treatment:
https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-5-75
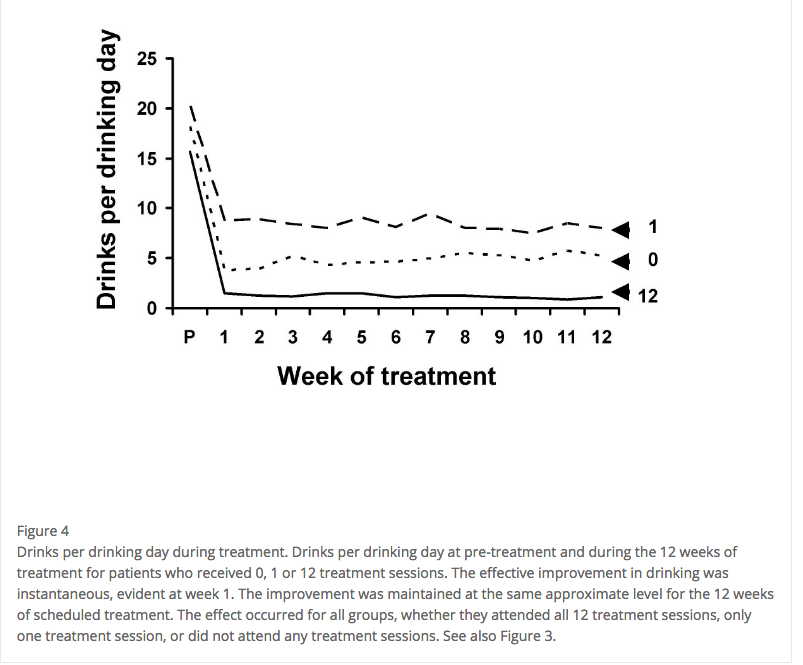
A similar reduction in drinking was found across groups that attended 12, 4, 1, or even ZERO weeks of treatment. The most important part of the results is that the reduction in drinking occurred between intake and the first treatment session a week later – people quit on their own, not as a result of the treatment.
Some would say, and have said that “the good news is all of these treatments are effective”, but I would say it shows none of them are effective, and it definitely flies in the face of the idea that continuing engagement in treatment is better. It’s not. Also, pay special attention to the charts at the bottom of the paper when you look at it, like this:
I took the time to write all of this back to you, because you obviously care about effectively helping people, so being informed of some other info about addiction can only help you to help others better.
Our goals of helping people are similar I’m sure, but the positions of your organization are in direct opposition to mine, so I’m sure we couldn’t work together at this point, and I wanted to explain why.
Best,
Steven